ANTONIO GUARNIERI
INGUINAL HERNIA
AND
PHYSIOLOGICAL HERNIOPLASTY
Contributors
Francesco Guarnieri,
MD, Clinica GUARNIERI - Rome
Enrico Nicolò, MD, FACS, UPMC- Pittsburgh,
PA. USA
Drawings by Mariacarla
Santorelli.
Translation from Italian by Kay
McCarthy
CENTRO STUDI CLINICA GUARNIERI
Via Tor de' Schiavi 139 00172 ROME
1999

INDEX
Introduction
PART ONE - CURRENT TECHNIQUES
1. Surgical anatomy notes.
The external oblique aponeurosis. The cribriform fascia.
The internal oblique muscle. The transversus muscle. The aponeurosis of
the transversus muscle and transversalis fascia The deep inguinal
ring. The spermatic cord. The preperitoneal tissue and peritoneum. The
vessels. The nerves. The femoral canal and the Cooper ligament. References
2. Approaches
The inguinal approach. The laparoscopic approach. Comments.
References.
3. Treatment of the sac
Isolation of the sac. Resection of the sac. Abandonment
of the sac. Comments. References
4. Repair techniques
through direct sutures
The Bassini repair technique. The Postempski or Halsted
repair. The McVay repair. The Shouldice repair. The Marcy repair. References.
5. Mesh repair
The Rives technique. Lichtensteins "tension free" hernioplasty.
The sutureless "Mesh-Plug" technique. The Stoppa technique (with giant
extraperitoneal mesh). The Wantz preperitoneal technique. The Nyhus technique.
Laparoscopic hernioplasty. References.
PART TWO PHYSIOLOGICAL HERNIOPLASTY
6. A reexamination
of the inguinal region from an anatomical and functional point of view
The anatomical and functional aspects of the anterior
abdominal wall. The structural aspects of the main anatomical layers of
the inguinal region in normal conditions and in hernia patients. The normal
defense mechanisms of the inguinal region (sling, sphincter and shutter
mechanisms). The functional aspects of the inguinal region in hernia patients.
Deductions. The myopectineal orifice.
7. Why a new method?
8. Physiological hernioplasty
The technique. The suture materials. The main technical
details.
9. The use of meshes
The use of preperitoneal meshes in primary hernias. The
use of meshes in the prefascial area in primary hernias. The use of meshes
in large inguinal and crural hernias. The use of the meshes in crural hernias.
The Locked-Plug technique. The use of meshes in inguinal recurrences.
10. Cases and results
Primary direct and indirect hernias. Recurrent hernias.
Locked-Plug. Follow-up.
11. Rationale
The elimination of the deep and formation of the new
ring. The narrowing and shortening of the inguinal canal. Overlapping the
external oblique aponeurotic flaps. Preservation of the cremaster. Discussion.
References
APPENDIX
12. The "Sandwich"
technique in incisional hernias
Incisions. Treatment of the sac. The "Sandwich" repair.
INTRODUCTION
INDEX
Widespread and easily tolerated, the inguinal hernia is
seen as a minor disorder. Because hernia surgery may be performed easily
and successfully in both in- and out-patient environments it is too often
dismissed as a trivial complaint. On the other hand, in many countries
it is considered a specialization. Unless inguinal hernia is treated properly,
in fact, it may turn out to be very disabling. Furthermore, international
statistics show that recurrences exceed the 10% mark. This means high social
costs. In Italy the number of hernia operations per annum stands around
100,000. Recurrent hernia surgery presents a higher relapse risk rate than
primary surgery. Repeated operations may also represent a hazard for the
testicular vessels.
The fact that the solution to the problem is by no means
straightforward is reflected in the existence of about 80 techniques, of
which over 20 currently in use.
Modern hernia surgery came
to the fore in Italy in 1884 with Edoardo Bassini. His technique, based
on the reconstruction of normal anatomical conditions, is one of the most
frequently performed techniques in use even today, perhaps because it is
easy to carry out despite its limits. It eliminates the physiological mechanisms
that defend the inguinal region from the stress of endoabdominal pressure
and creates a cicatricial barrier. However, in large hernias, excess suture
traction remains and the risk of recurrence is high.
Prosthetic surgery. Since the end of the
1950's, biocompatible meshes have provided hernia surgery with noteworthy
advantages. The primary benefit of prosthetic surgery is that weak tissue
is replaced and suture tension eliminated. Although many surgeons advocate
the employment of prosthetic meshes they have not as yet been universally
accepted. Effectively speaking, the use of foreign bodies, that is, meshes,
in all hernias does appear too much of an exaggeration.
Physiological hernioplasty is the name
I have given to the technique I outline here. At the end of the 1980's,
having used various techniques, with and without mesh, I grew dissatisfied
with the cicatricial barrier produced by traditional techniques and with
overuse of prostheses. So, I began to seek a new solution.
My primary goal was to reconstruct the physiology
by reactivating the inguinal regions muscular defense mechanisms.
The inguinal region is a notoriously weak area because it is crossed by
the tunnel containing the spermatic cord running through prevalently fascial
tissue. On the contrary, where muscle tissue exists, there is no hernia
because this tissue contracts and hardens when endoabdominal pressure increases.
In hernia patients the muscles of the inguinal region are nearly always
hypotrophic and the inguinal canal altered. I thought of the possibility
of modifying the anatomic structure of the inguinal region so that it might
be adapted to the needs of physiology. It was clear to me that any
attempt at repairing the deep ring would be a failure because the tissue
surrounding it is particularly weak in hernia patients. Therefore, I thought
of closing the ring completely and creating a totally new one at the same
anatomic level, but more medial than the original and in a stronger area.
At the same time, it occurred to me that the external oblique aponeurosis
might be exploited as an extraordinarily efficacious biological "prosthesis"
to reinforce the non-muscle zones and modify the dimensions of the inguinal
canal which could then be adjusted to the muscular tissue. In December
1988 I began to make use of this method. Since then, we have operated on
over 2,000 inguinal hernia patients.
The results have been successful. The incidence of recurrence
stands at about 0.6 % for primary hernias and most of the operations have
been performed in local anesthesia. The meshes used as reinforcement in
primary hernias were availed of only in the presence of very poor tissues,
that is, about 5% of the time.
All the research and clinical work has been carried out
in two private hospital departments: the CLINICA GUARNIERI and ARS MEDICA
in Rome. This is rather unusual for Italy where most research is carried
out in public hospitals and in university clinics.
I wish to thank all my collaborators: doctors, technicians,
and my staff of nurses, clerks and assistants. They are all wonderful people
indeed.
This book is not a new edition of my previous "La
nuova chirurgia dell'ernia" (Masson 1995) but rather a condensed and
updated version of it.
It is intended for the surgeons of today but above all
for those of tomorrow who, maybe, when enthusiasm for prostheses dies down
and old methods grow even older, will judge my proposal with greater serenity
and equilibrium.
Rome, August 1999
ANTONIO GUARNIERI
INDEX
1
SURGICAL ANATOMY NOTES
INDEX
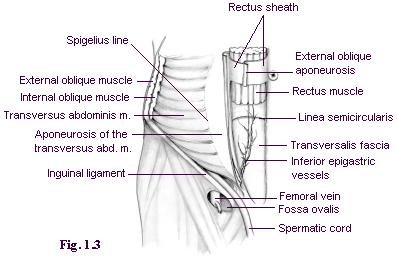
The external oblique aponeurosis (Fig. 1.1)
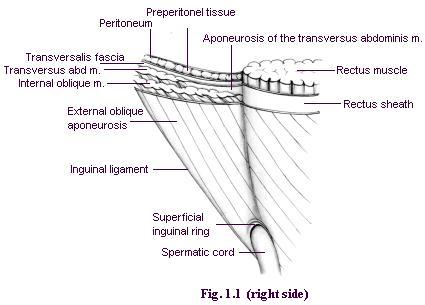
The external oblique aponeurosis is the front
wall of the inguinal canal and, at its lateral and lower location, is the
continuum of the inguinal ligament. The superficial inguinal ring is the
passage through which the spermatic cord passes and is covered by a thin
membrane - the external spermatic fascia. The external oblique aponeurosis
is joined medially to the aponeurosis of the internal oblique and transversus
muscles, forming the medial half of the anterior rectus sheath (Fig. 1.3).
The lateral half of the rectus sheath is simply covered by the external
oblique aponeurosis, from which it may be separated with greater or lesser
ease.
Contraction of the external oblique muscle stiffens the
aponeurosis and causes a narrowing of the superficial ring.
The cribriform fascia
This is a thin layer that occludes the fossa ovalis.
It is the continuation of the femoralis fascia and is joined to
the external oblique aponeurosis. It covers the femoral canal from which
it is separated by lax fatty tissue.
The internal oblique muscle (Fig. 1.2)
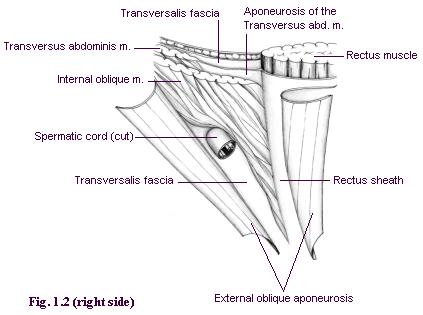
Below the external oblique aponeurosis lies a lower layer.
Medially, it consists of the lateral side of the rectus sheath, originating
from the fusion of the aponeurosis of the internal oblique muscle and the
transversus muscle. Continuing laterally we find the internal oblique muscle
which usually borders on the rectus sheath and sometimes covers it completely.
Only the inferior part of the internal oblique muscle
is a part of the inguinal region. It covers the transversus muscle and
its aponeurosis. The lower fibers of the internal oblique muscle form an
arch that circumscribes the funiculus along the inguinal canal. The inferior
border of the internal oblique muscle normally reaches the pubic spine.
In hernia patients, the insertion of the inferior edge of the internal
oblique muscle often reaches the rectus sheath in a position rather high
compared to the pubic spine. The result is a triangular zone surrounded
by the inferior border of the internal oblique muscle, by the inguinal
ligament and by the lateral border of the rectus sheath. Thus, this area,
called the inguinal triangle (see Fig.
6.3), is not defended by the internal oblique muscle, which gives rise
to a tendency to yield and produce direct hernias. The inguinal triangle
must not be confused with the Hesselbach triangle which is surrounded
by the inguinal ligament, inferior epigastric vessels and the lateral border
of the rectus muscle.
The transversus muscle (Fig. 1.3 - 1.4)
The transversus muscle follows the same path as the internal
oblique muscle, is located deeper and is less present in the inguinal region
than the latter. The inferior edge of the muscular part does not, in most
cases, reach the midpoint of the inguinal ligament. In 26% of all cases
it does not go beyond the anterior superior iliac spine. Medially too this
muscular portion ends at a certain distance from the rectus muscle. The
transversus muscle at inguinal canal level is scarcely represented.
The aponeurosis of the transversus muscle and transversalis fascia
The deep inguinal ring (Fig 1.4)
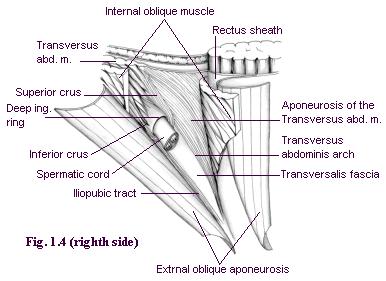
The anterior aponeurosis of the transversus muscle and
the transversalis fascia are practically joined together and represent
the posterior plane of the inguinal region. To be exact, the aponeurosis
of the transversus forms an arch, called the aponeurotic arch of the
transversus, which coincides substantially with the arch of the internal
oblique muscle. Therefore, the posterior wall of the canal, behind the
funiculus, consists of a layer, the transversalis fascia, which is reinforced
laterally by the iliopubic tract and medially by the aponeurotic arch of
the transversus. The aponeurotic arch of the transversus should not be
confused with the semilunar line of Spigelio (Fig 1.3) that is, the border
between the muscular and the aponeurotic part of the transversus which
runs from the hypochondrium to the inguinal region. Cranially and laterally,
the deep ring is bordered on by the transversalis fascia and transversus
muscle or by its aponeurosis. Medially and caudally, it borders on the
plane comprising the aponeurosis of the transversus + transversalis fascia,
which in this tract presents a sling-shaped thickening. The two ends of
this thickening are called, respectively, inferior and superior crura.
The inferior crus, the shorter of the two, is positioned laterally, joining
the iliopubic tract. The superior crus, which is longer, is directed upwards,
laterally and backwards, forming a flap on the fascia transversalis to
the inner side of the deep ring.
Medially, the aponeurosis of the transversus muscle joins
the aponeurosis of the internal oblique muscle to form the anterior part
of the rectus sheath while the trasversalis fascia passes behind the rectus
muscle. Laterally, along the angle of the transversalis fascia and the
inguinal ligament, there is a thickening, the iliopubic tract. At
a deeper level, the transversalis fascia joins the femoral vessels and
the Cooper ligament, and forms the femoral septum that occludes the crural
ring.
The contraction of the transversus muscle attracts
the superior crus upwards and laterally and, with it, the fold of the transversalis
fascia which covers the deep ring from the inside (sling effect) like an
eyelid. The inferior crus is fixed. The deep ring, besides being covered
posteriorly, is tightened by the fibers of the aponeurosis of the transversus
and pulled upwards and outwards. When the muscles contract, the deep ring
passes under the internal oblique muscle which is simultaneously tended
and lowered. This protection mechanism is called the "sphincter mechanism".
The simultaneous contraction of the internal oblique
and transverse muscles creates the Keith shutter mechanism, which protects
the posterior wall of the inguinal canal from endoabdominal pressure. As
a result of the contraction, the internal oblique muscle stiffens and becomes
shorter; the arch straightens, lowers and leans on the inguinal ligament.
The same happens to the aponeurotic arch of the transversus muscle.
The spermatic cord
The most important elements of the spermatic cord are:
the deferent duct, the deferential artery, the testicular artery, the pampiniform
plexus. These elements are enveloped by the internal spermatic fascia which
forms a continuum with the transversalis fascia. Externally we find the
cremaster. The cremaster is the continuum of the internal oblique muscle
and pulls the testicle up towards the superficial inguinal ring. The genital
branch of the genitofemoral nerve innervates it. It is vascularized by
the funicular artery, a branch of the inferior epigastric artery.
In women the content of the inguinal canal is the round
ligament accompanied by some unimportant vessels (artery of the round ligament)
and by nerves (iliohypogastric, ilioinguinal, and genitofemoral).
The preperitoneal tissue and the peritoneum
The preperitoneal tissue is mostly fat and is located
between the transversalis fascia and the peritoneum. It is easily separable
from the transversalis fascia.
The vessels
The inferior epigastric vessels,(artery and two
veins) stem from external iliac vessels. They pass by the deep inguinal
ring, below and medially with respect to it, and proceed obliquely towards
the posterior surface of the rectus muscle. The vessels are located between
the peritoneum and the transversalis fascia. At times they adhere to the
transversalis fascia. It is advisable not to section and tie the inferior
epigastric vessels, but in cases of hemorrhage or when a prosthesis has
to be positioned, this may be done with the utmost tranquillity.
The funicular vessels stem
from the inferior epigastric vessels and reach the funiculus through the
deep ring or a small hole directly under this, coming very close to the
transversalis fascia.
The iliac and femoral vessels pass through the lacuna
vasorum. They are easily recognizable in laparoscopic surgery. In traditional
hernia surgery risk of lesion to these big vessels is quite remote. But
excessive stenosis of a crural hernial defect during repair may cause compression
of the femoral vein, which is located medially to the artery and is often
more easily detected through palpation than at sight.
The nerves
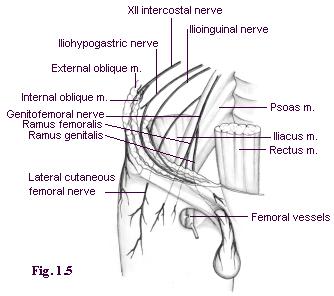
The nerves (Fig. 1.5) of greatest interest are:
- The terminal cutaneous branches of the XI and XII
intercostal nerves.
- The genital branches of iliohypogastric and ilioinguinal
which run parallel to each other. The iliohypogastric nerve runs above
the ilioinguinal one before turning medially. At the iliac crest they pass
between the transversus and the internal oblique muscles. In the inguinal
canal they are located between the internal oblique muscle and the external
oblique aponeurosis together with the funiculus.
During hernia surgery, the subcutaneous terminal branches,
which pass through the external oblique aponeurosis, can sometimes complicate
the mobilization of this layer. It is necessary to isolate them; if, on
account of their position, they run the risk of being strained or becoming
tangled in the suture they should be sectioned to avoid postsurgical
pain.
- The lateral external cutaneous nerve and the femoral
branch of the genitofemoral nerve innervate the skin of the thigh laterally
down to the knee as well as the skin on the upper part of the "Scarpa triangle".
These are rather marginal to the area operated during hernia surgery.
- The genital branch of the genitofemoral nerve
penetrates the inguinal canal through the deep ring. Together with the
funicular vessels, it runs posterior to the funiculus and innervates the
cremaster. It then exits through the superficial ring and innervates the
skin of the scrotum or the major labium as well as the superomedial part
of the thigh.
These nerves are almost all sensory nerves. The only
motor nerve is the genital branch of the genitofemoral nerve, which innervates
the cremaster.
It is important to know the nerve path well, not only
to perform in local anesthesia but also because, if cut or caught up in
the stitches hypoesthesia or postoperative pain, respectively, may be caused.
One may say that even when these nerves are cut the ensuing, hypoesthesia
diminished over time and is confined ultimately to small skin areas.
The femoral canal and the Cooper ligament (Fig. 1.6)
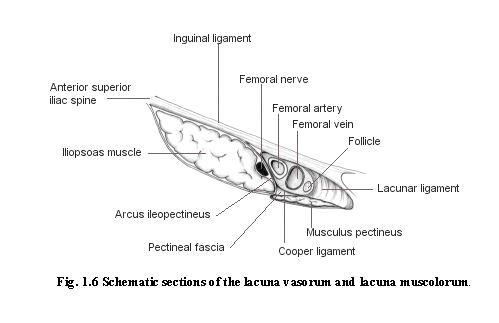
The femoral or crural canal is delimited:
- anteriorly, by the iliopubic tract and immediately
to the front by the ilioinguinal ligament
- medially, by the Gimbernat ligament and the recurved
portion of the iliopubic tract at its insertion into the area of Cooper.
- posteriorly, by the pectineal fascia, which, at the
level of the pectineal line, grows thicker and is called the Cooper ligament
- laterally, by the arcus ileopectineus which covers
the psoas muscle and separates the femoral nerve from the femoral vessels.
Medially to the vein, the femoral canal is closed by
the transversalis fascia, which at this point is known as the septum femorale,
and is crossed by a number of lymphatic vessels. Crural hernias generally
occur medially to the femoral vein due to weakness in the femoral septum;
less frequently prevascular hernias are known to occur.
INDEX
References
ANSON B.J., Mc VAY C.B.: The anatomy of the inguinal and
hypogastric regions of the abdominal wall. Anat.Rec.70: 211-225,1938.
ANSON B.J., Mc VAY C.B.: Inguinal hernia. The anatomy
of the region. Surg. Gynecol. Obstet. 66: 186-191, 1938.
CONDON R.E.: Surgical anatomy of the transversus abdominis
and transversalis fascia. Ann. Surg. 173:1,1971.
FRUCHAUD H.: Anatomie chirurgicale des hernies de l'aine.
G. DOIN, edit., Paris, 1956.
GLASSOW F.: The Shouldice repair for inguinal hernia.
In. NYHUS L.M., CONDOM R.E. (Eds): Hernia. J.B. Lippincott Co., Philadelphia,
2nd ed., 1978.
HESSELBACH F.C.: De ortu herniarum. Wurzberg, Stael 1816,
cited by LYTLE W.J., Br. J.Surg. 57: 531, 1970
KEITH A.: On the origin and nature of hernia. Br. J.
Surg. 11:455, 1924
LYTLE W.J.: The internal inguinal ring. Br. J. Surg 32:
29, 1945
McVAY C.B., ANSON B.J.: Aponeurotic and fascial continuities
in abdomen, pelvis and thigh. Anat. Rec. 70: 213-231, 1940.
POLJA E.: Die Ursachen der Rezidive nach Radikaloperation
des Leistenbueche. Zentr. f. Chir. 30: 816, 1912
ROUVIERE H.: Anatomie humaine. Masson, Paris, 1962
RUTLEDGE R.H.: Cooper's ligament repair for adult groin
hernias. Surgery 87: 601-610, 1980
TESTUT L., JACOB O.: Anatomia topografica. UTET, Torino,
1950
ZIMMERMAN L.M.: The surgical treatment of direct inguinal
hernia. Surg. Gynecol. Obstet. 66: 192-198, 1938
2
APPROACHES
INDEX
All modern hernia surgery consists in three phases:
- reaching the sac and the hernia defect
- treating the sac
- repair
The sac and the hernia defect may be reached through
three different surgical approaches: inguinal, preperitoneal and transperitoneal.
The inguinal approach
The inguinal approach is the most direct. The hernia defect
may be reached anteriorly in two ways: 1) through an oblique incision in
the skin, parallel to the groin, and medially, at about a distance of two
fingers from it, or 2) by a transverse incision at deep inguinal ring level.
The external oblique aponeurosis is cut following the
grain of the fibers and the superficial ring is opened.
The spermatic cord is isolated starting from the pubic
spine and drawn back laterally.
In indirect hernias, the sac is isolated from the elements
of the spermatic cord, once the internal spermatic fascia has been opened.
In direct hernia, the sac is reached easily after cutting the transversalis
fascia on the back wall of the inguinal canal.
The preperitoneal approach
The hernia defect may be reached from behind through the
preperitoneal space. Today these approaches have been reevaluated thanks
to the advent of laparoscopy.

The most common skin incisions currently used are the
following (Fig. 2.1):
- midline umbilico pubic;
- transverse suprapubic according to the Pfannenstiel
method;
- suprainguinal transversal, two fingers above the symphysis
pubis.
The first two types of incisions allow simultaneous treatment
of bilateral hernias.
Dissection of the deep layers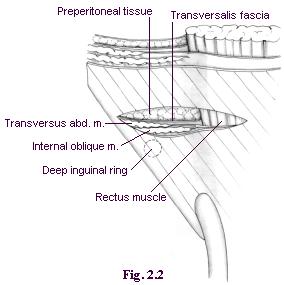
Through a midline incision, passing through the two rectus
muscles, the preperitoneal tissue is reached.
In the Pfannenstiel incision, the sheath of the rectus
muscles is cut transversally and detached from the underlying level.
The peritoneum is then separated from its wall until
the affected inguinal area is reached. The epigastric vessels remain attached
to the wall.
The suprainguinal incision must be executed slightly
above the deep ring. The incision is made transversally along the rectus
sheath starting from the midline and across the internal oblique and the
transversus muscles. This way the transversalis fascia may be reached (Fig.2.2).
The lateral edge of the rectus muscle is retracted towards
the midline. Then the transversalis fascia may be cut longitudinally down
the lateral edge of the rectus muscle or, as Nyhus proposes, transversally,
to reduce herniation of the wound. Under no circumstances should the peritoneum
be cut. This incision leads to the inferior epigastric vessels which, normally,
must be interrupted and tied.
Then, continuing to separate the peritoneum from the
wall, the hernial sac is reached.
The laparoscopic approach
Enrico Nicolo'
Even if an intraperitoneal laparoscopic approach exists,
a preperitoneal one is generally preferred.
The preperitoneum may be reached directly, without opening
the peritoneum, as well as transperitoneally.
In the latter case, the hernia defect may be reached
through the inner side of the abdomen cavity by an incision on the parietal
peritoneum which will later be sutured.
The laparoscopic approach requires specific experience
and a good "inside" knowledge of anatomy.
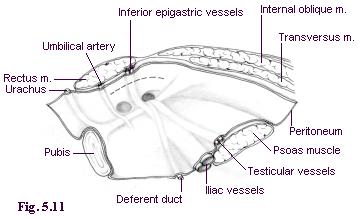
(See Figs. 5.11 and 5.12).


The transabdominal preperitoneal approach
After having performed a pneumoperitoneum, a laparoscope
with a 30-degree view is introduced through the umbilicus. Two trocars
are inserted at the lateral edge of the rectus muscle, one on the left,
the other on the right, at umbilical level (Fig. 2.3).
The totally extraperitoneal approach
A vertical incision, 1-2 cm long, under the umbilicus
and 1 cm lateral to the linea alba, on the side opposite to the hernia,
is made. (Fig. 2.4). The anterior rectus sheath is cut, the muscle is retracted
and a special balloon probe, which slides along the posterior sheath of
the rectus muscle until it reaches the pubic bone, is inserted. The optics
are inserted, the balloon is inflated to separate the preperitoneum. After
3-4 minutes, the optics are removed. The balloon is deflated and the probe
is removed. Through the same hole, a sealed trocar is introduced and carbon
dioxide blown in. Two trocars are inserted at the midline, one above the
pubis, the other half way between the umbilicus and pubis (Fig.2.4).
Comments
The inguinal approach
This is undoubtedly the most frequently chosen.
Advantages:
- the possibility of performing under local anesthetic
- direct and easy access on all anatomic levels
- very low risk of lesion of large vessels.
Disadvantages:
- difficult dissection in hernia recurrence with added
risk of lesion to testicular vessels
- frequent traumatism of the inguinal canal nerves with
consequent hypoesthesia and neuralgia
The preperitoneal approach
In many cases this requires a general anesthetic, except
in the case of suprainguinal incisions.
Advantages:
-in hernia recurrences, the difficult dissection of the
scar tissues is avoided. The risk of testicular vessel lesion is reduced.
-elimination of inguinal canal nerve traumas
-the possibility of treating hernia during operation
for other pathologies
-bilateral hernias may be treated simultaneously if a
midline incision is performed
Disadvantages:
- limited possibility of performance in local anesthetic
- increased width and depth of the operating field compared
to the inguinal approach
- impossibility of reaching surface layers of the inguinal
region
- practically imperative use of prosthesis due to the
poor results with use of direct suture and to avoid risk of hernia on the
wound.
The laparoscopic approach
Perhaps, because it is very recent, it is still too soon
to express a proper evaluation of this new approach and when it is indicated.
Problems of training, the development of new methods and instruments are
still being addressed. On the one hand, enthusiasm for novelty and the
strong influence of the biomedical industry are keenly felt, but on the
other, distrust towards new and more sophisticated techniques exists, also
because these techniques are difficult to acquire.
Those who advocate this method assert that the risk of
trauma is low, that postoperative pain is slight, that immediate resumption
of physical activity is possible and that no risk of ischemic orchitis
exists. The criticism this technique arouses is similar to that for extraperitoneal
techniques.
Concluding, the inguinal approach is still the most frequently
chosen. Only in particular cases are different approaches preferred.
Cases in which preperitoneal or laparoscopic approaches
are indicated:
- complicated and multiple hernia recurrence
- bilateral hernias to be treated simultaneously
- treatment of hernia during operations for other ailments.
INDEX
References
CALNE R.Y.: Repair of bilateral hernia, a technique using
Mersilene mesh behind the rectus abdominis. Br. J. Surg. 54: 917, 1967
CHEATLE G.L.: An operation for the radical cure of inguinal
and femoral hernia. Br. Med. J. 2: 168.1920
COPELLO A.J. :Technique and results of Teflon mesh repair
of complicated recurrent groin hernias. Rev. Surg. 25: 95,1968
ESTRIN J. et al.: The posterior approach to inguinal
and femoral hernia. Surg. Gynecol. Obstet. 116: 547, 1963.
HENRY A.K.: Operation for femoral hernia by a midline
extraperitoneal approach. Lancet. 1: 531, 1936
JENNINGS W.K., ANSON B.J.: A new method of repair for
indirect inguinal hernia considered in reference to parietal anatomy. Surg.
Gynecol. Obstet. 74: 697, 1942
McEVEDY P.G.: Femoral hernia. Ann. R. Coll. Surg. Eng.
7: 484, 1950
McNAUGHT G.H.D.: Femoral hernia: the rectus sheath operation
of McEvedey. J. Coll. Surg. Edinb. 1:309, 1956
MIKKELSEN W.P., BERNE C.J.: Femoral hernioplasty: suprapubic
extraperitoneal (Cheatle-Henry) approach. Surgery 35: 743, 1954
MOSCHOWITZ A.V.: Femoral hernia: A new operation for
the radical cure. N.Y State J. Med. 7:396, 1907
MUSGROVE J.E., McCREADY F.J. The Henry approach to femoral
hernia. Surgery 26: 608, 1949
NYHUS L.M. et al.: Preperitoneal herniorrhaphy: A preliminary
report in fifty patients. West J. Surg. Obstet. Gynecol. 67: 48, 1959
NYHUS L.M. et al.: The preperitoneal approach and prosthetic
buttress repair for recurrent hernia: the evolution of a technique. Ann.
Surg. 208: 733-737, 1988
NYHUS L.M.: Inguinal hernia. Curr. Prob. Surg XXVIII-6:
406-450, 1991
NYHUS L.M.: The preperitoneal approach and iliopubic
tract repair of inguinal hernia. In: NYHUS L.M., CONDON R.E. (eds.): Hernia.
J.B: Lippincott Co., Philadelphia, 3rd. ed., 1989, pp 154 -198
READ R.C.: Preperitoneal exposure. Curr. Prob. Surg.
4. 17, 1967
READ R.C.: Preperitoneal herniorrhaphy: a historical
view. World J. Surg. 13: 532-540, 1989
READ R.C.: Preperitoneal prosthetic inguinal herniorrhaphy
without a relaxing incision. Am. J. Surg. 132: 749, 1976
REAY-YOUNG P.S.: Repair of femoral hernia. Lancet 2:
1217, 1956
STOPPA R. et al.: Unsutured Dacron prosthesis in groin
hernias. Int. Surg. 60: 411, 1975
WANTZ G.E.: Giant prosthetic reinforcement of the visceral
sac. Surg. Gynecol. Obstet. 169: 408, 1989
3
TREATMENT OF THE SAC
INDEX
The hernial sac is an outward bulging of the parietal
peritoneum. The sac itself consists of a neck, a body and a fundus. The
neck is the proximal portion surrounded by the hernia defect.
Isolation of the sac
For more than a century the necessity to isolate the sac
from the transversalis fascia beyond the neck has been known.
Through the inguinal approach, the isolation of
the sac in direct hernias is quite straightforward. In indirect hernias,
sometimes the sac may reach the scrotum or adhere to the funiculus. In
these cases wide dissection should not be performed because it might provoke
distal vein thrombosis and ischemic orchitis: the sac may be isolated from
the neck up to the pubis and divided at this point. The body and the fundus
may be left in situ.
The preperitoneal approach: in direct hernias
the isolation of the sac is again straightforward; in indirect hernias,
the sac is easily isolated by applying medium traction on the peritoneum.
In case of stubborn adhesions the sac may be divided at the level of the
neck and left in situ.
Resection of the sac
Having isolated the sac beyond the neck, the complete
resection and closure, with ties or high suture of the sac, are carried
out in the traditional manner.
Alternatively, after the resection of the sac, the peritoneal
gap may be left unsutured. Some authors hold that this does not cause additional
complications because the peritoneum heals immediately and completely.
Postoperative pain should be less because less phlogosis of the parietal
peritoneum occurs.
Abandonment of the sac
The abandonment of the sac, without even opening it, in
the preperitoneal space may be performed in both direct and indirect hernias.
Abandonment causes multiple folding of the walls and an effective elimination
of the sac, which will not expand.
Comments
Personally, I prefer the abandonment of the sac in the
preperitoneum which practice is possible in most cases. I tend to avoid
ties when the sac has to be divided to prevent traumatic separation of
the body and fundus.
Abandonment of the sac, which I have performed during
thousands of operations, is easy and safe because there is no risk of viscera
lesion, which may occur in cases of resection. When this not too rare kind
of viscera lesion occurs it usually involves the bladder. In any case,
the opening of a sac with thick walls and /or in the presence of sliding
hernia may create problems. Another advantage related to sac abandonment
is that postoperative pain is reduced noticeably.
INDEX
References
FERGUSON D.J.: Closure of the hernial sac. Pro and Con.
In NYHUS L.M., CONDOM R.E. (eds): Hernia 2nd ed., J.B. Lippincott Co.,
Philadelphia, 1978, pp. 152-153
SAM G.G. et al.: Ligation of the hernial sac? Surg. Cl.
North Am. 64: 299-305, 1984
SHULMAN A.G. AMID P.K: LICHTENSTEIN I.L.: Ligation of
hernial sac a needless step in adult hernioplasty. Int. Surg. 78: 152-153,
1993
WANTZ G.E.: Testicular atrophy as a risk of inguinal
hernioplasty. Surg. Gynecol. Obstet. 154: 570-571, 1982
4
REPAIR TECHNIQUES
THROUGH DIRECT SUTURE
INDEX
Repair may be performed either by suturing the anatomic
layers (herniorrhaphy) or by inserting a biocompatible mesh in order to
reinforce the tissues (prosthetic hernioplasty). The tissues themselves
may be used for the same purpose (hernioplasty).
The Bassini, Postempski, McVay, Shouldice and Marcy
techniques are all performed availing of the inguinal approach and
are the most frequently used at present.
The Bassini repair
 In
order to perform the Bassini technique correctly, the resection of the
cremaster and an incision of the transversalis fascia from the deep inguinal
ring to the pubic spine are mandatory. These phases are often omitted and
wrongly so. The repair of the inguinal canal takes place upon two planes.
The deep layers are sutured using separate stitches one centimeter apart.
The suture starts from the pubis and medially includes three layers: the
internal oblique muscle, the aponeurosis of the transversus muscle and
transversalis fascia; laterally, the iliopubic
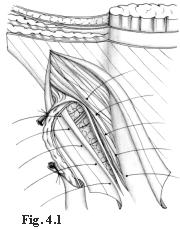
In
order to perform the Bassini technique correctly, the resection of the
cremaster and an incision of the transversalis fascia from the deep inguinal
ring to the pubic spine are mandatory. These phases are often omitted and
wrongly so. The repair of the inguinal canal takes place upon two planes.
The deep layers are sutured using separate stitches one centimeter apart.
The suture starts from the pubis and medially includes three layers: the
internal oblique muscle, the aponeurosis of the transversus muscle and
transversalis fascia; laterally, the iliopubic
tract and the inguinal ligament (Fig. 4.1).
The suture reaches the deep ring, which is tightened
in such a way as to avoid compression of the cord vessels.
Once the funiculus is placed to the front of this suture,
the external oblique aponeurosis is sutured.
At lower level the "joined tendon" is not always well
represented. In this case the first stitches are placed on the rectus sheath.
Principles of the technique
Bassini's intention was to reconstruct the normal anatomy.
Mistakenly, he believed it would also reestablish the normal physiological
defense mechanisms, which he believed depended on the obliqueness of the
canal and the level variation between the superficial and deep rings.
Comments
On no other technique has so much been written. Many
surgeons continue to believe strongly in this technique, even if the reported
results are both good and bad. This ambiguity may be due to incomplete
follow-up, good/bad execution of the technique, the experience/inexperience
of the surgeons. What is unquestionable, though, is the high incidence
of recurrence (about 10%).
The incidence of recurrence may be considered the most
noticeable drawback of the Bassini technique, although there are others.
Above all, physiology is not respected; in fact, the
deep inguinal ring, anchored to the inguinal ligament, loses its mobility
and its normal defense mechanisms. The transversus and internal oblique
muscles are united, while in normal conditions each of them moves independently
and complementary to the other (sphincter effect).
Moreover, the technique does not follow principles of
tissue synthesis:
- the stitches that pass through the entire wall may
rupture the tissue and create new hernia defects.
- the muscles are not usually fit for sutures: they rupture
easily, lose motility and form scar tissue.
- the suture between the rectus sheath and inguinal ligament,
performed when the internal oblique muscle is atrophic, is under strong
traction due to poor tissue elasticity.
Because it is known and performed worldwide, the advantages
of the Bassini technique are that it is easily performed and learnt.
The Postempski or Halsted Repair
This method differs from that of Bassini in one way: the
repair of the external oblique aponeurosis occurs behind the funiculus.
The superficial ring is located upwards and aligned with the deep ring.
The funiculus is made to run through the subcutaneous tissue.
Principles of the technique
This technique aims at eliminating the weak point in
the Bassini technique (the inferior area) and at creating a scar wall formed
by the fusion of the posterior and anterior layers.
Comments
This technique creates a reliable reinforcement of the
weak zone near the pubic spine but creates alignment between two weak points:
the superficial and deep rings. This alignment has been criticized because
it eliminates the defense of the external oblique aponeurosis on the deep
ring, already deprived of the sphincter effect. Nevertheless, the incidence
of recurrence is lower in Postempskis technique than in Bassini's. Recurrences
of direct hernia at the inferior angle are very rare, while those of indirect
hernia are the same as in Bassini. These results are obvious, since the
external oblique aponeurosis supports the levels below. The risk of recurrence
is linked to the resistance of the deep layers and to the deterioration
of the physiological defense mechanisms.
The McVay repair
 This
technique is in keeping with current inguinal and crural hernia therapy
and with the supporters of the Fruchaud thesis on the need (on principal)
to treat the myopectineal orifice. Lotheissen devised it in 1897, but without
practicing a relaxing incision on the rectus sheath; the suture traction
was excessive.
This
technique is in keeping with current inguinal and crural hernia therapy
and with the supporters of the Fruchaud thesis on the need (on principal)
to treat the myopectineal orifice. Lotheissen devised it in 1897, but without
practicing a relaxing incision on the rectus sheath; the suture traction
was excessive.
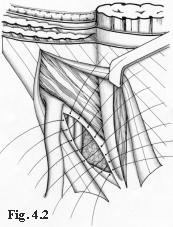
The transversalis fascia must be opened as far as the
pubis to reach the Cooper ligament. Repair occurs on two layers. The deep
layer is created, using interrupted stitches to join the transversus aponeurosis
+ transversalis to the Cooper ligament as far as the femoral vein, which
should not be compressed. Then, the aponeurotic layer is sutured to the
femoral sheath and to the iliopubic tract as far as the deep ring. A relaxing
incision on the rectus sheath is performed in advance to avoid excessive
suture tension. (Fig. 4.2). The inguinal ligament and the internal oblique
muscle are not involved in the suture.
The funiculus is relocated on this layer and the external
oblique aponeurosis sutured.
Principles of the technique
This technique aims at anatomical repair of the whole
myopectineal orifice: in fact the Cooper ligament is considered the perfect
continuation of the transversalis fascia.
Comments
This technique respects both anatomy and physiology, because
it does not compromise the motility of the deep ring and internal oblique
muscle. But the repair of the deep ring does not guarantee solidity, therefore
an indirect hernia may form. Frequently, repair is not well performed because
the transversalis fascia near the deep ring is often dystrophic and very
thin. The suture between the transversalis fascia and aponeurosis of the
transversus muscle and the Cooper ligament seems unreliable, because it
may come under tension. Also, the thin aponeurotic layer, if not protected
sufficiently by the internal oblique muscle, may yield.
Nevertheless, this technique proves more successful than
Bassini's. The incidence of recurrence has been shown to vary from 3.5%
to 7.5%. I think that these results are linked to the fact that physiology
is respected and that the rectus muscle may expand laterally. As a consequence,
the weak zone is reduced.
The Shouldice repair
 Shouldice's
technique was devised between 1945 and 1953 optimizing the Bassini technique.
For example, suturing with an overlapping of the transversalis fascia (Harrison
1922).
Shouldice's
technique was devised between 1945 and 1953 optimizing the Bassini technique.
For example, suturing with an overlapping of the transversalis fascia (Harrison
1922).
Resection of the cremaster and opening of the transversalis
fascia from the deep ring to the pubic spine are mandatory as well as systematic
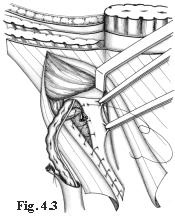
exploration of the crural ring. Repair is performed with three continuous
doubleline ("back and forth") sutures.
The first retrofunicular suture line joins the inner
surface of the transversalis fascia (close to the lateral margin of the
rectus muscle) to the iliopubic tract, beginning from the pubic spine up
to the deep ring. The suture reaches the deep ring, and includes the proximal
stump of the cremaster in order to repair and reinforce the ring (Fig.
4.3). On its way back, the second suture line joins the medial flap of
the transversalis  fascia
left over by the previous step to the inguinal ligament. In this way, a
suture with overlapping flaps of the transversalis fascia is obtained (Fig.
4.4). The second retrofunicular suture line, on the way out, joins the
margin of the internal oblique muscle to the inguinal ligament near the
previous level and on the way back includes the anterior surface of the
internal oblique muscle and the inner surface of the lateral flap of the
external oblique aponeurosis. Once the suture has been performed, the distal
stump of the cremaster is also included to sustain the testicle.
fascia
left over by the previous step to the inguinal ligament. In this way, a
suture with overlapping flaps of the transversalis fascia is obtained (Fig.
4.4). The second retrofunicular suture line, on the way out, joins the
margin of the internal oblique muscle to the inguinal ligament near the
previous level and on the way back includes the anterior surface of the
internal oblique muscle and the inner surface of the lateral flap of the
external oblique aponeurosis. Once the suture has been performed, the distal
stump of the cremaster is also included to sustain the testicle.
The funiculus is then replaced at this level.
A third doubleline continuous suture passes in front
of the funiculus and joins the margin of the lateral flap of the external
oblique aponeurosis and the inner surface of its medial flap, 2-3 cm from
the border. As it returns, the medial flap covers and is sutured to the
lateral one.
The original technique requires the use of steel thread.
This technique has undergone some changes: the abolition
of the third and fourth layers and the repair without overlapping of the
external oblique aponeurosis flaps. The results do not seem equally encouraging.
The principles of the technique
A series of improvements and changes concerning the tissue-synthesis
have improved the Bassini technique:
-
no suture tension occurs because the rectus muscle is mobilized,
-
sutures are not aligned and do not involve the whole wall,
-
scar surfaces rather than scar borders are produced,
-
the modeling of the deep ring, using the proximal stump of
the cremaster, is improved.
Comments
It should be observed that the second suture layer blocks
the deep ring on to the inguinal ligament, while the third and fourth layers
involve the internal oblique muscle completely. This means that physiology
is not respected at all.
On the other hand, tissue-synthesis is respected and
an accurate repair of the deep inguinal ring is achieved.
Results prove to be good. The incidence of postoperative
recurrence is lower than 1% in cases performed by the surgeons from the
Shouldice Clinic. According to them, to obtain these results, a five-year
training period is necessary.
The Marcy repair
The Marcy technique was published in 1871. Although a
century old, it still shows interesting characteristics although limited
in scope.
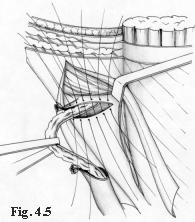
This technique implies the resection of the cremaster
and a careful exposition of the deep ring. Having treated the sac, the
ring is repaired and calibrated with a suture which medially recomposes
the transversalis fascia + transversus aponeurosis layer (Fig. 4.5). A
simple suture then repairs the external oblique aponeurosis.
Principles of the technique
This repair technique respects the normal anatomy and
physiology of the inguinal canal.
Comments
This techniques major defect is its lack of treatment
of the posterior wall of the inguinal canal.
This technique is suitable for indirect hernias and when
both the internal oblique muscle and the transversalis fascia are in good
condition, as in forms of congenital hernias in babies and youths. In such
cases, in fact, resection of the cremaster is not the best choice.
Surgeons very familiar with the deep ring may carry out
satisfactory repair availing of the Marcy technique without resecting the
cremaster; it suffices to separate the elements of the funiculus from the
proximal tract of the cremaster.
INDEX
References
ASMUSSEN T., JENSEN F.U.: A follow-up study on recurrence
after inguinal hernia repair. Surg. Gynecol. Obstet 156: 198-200. 1983
BARBIER J. et al: Traitment des hernies inguinales selon
la technique de Mc Vay. A propos de 1000 cas. Chirurgie 110: 144, 1984
BASSINI E.: Nuovo metodo operativo per la cura dell'ernia
inguinale. Padova, 1889.
BERLINER S.D., WISE L.: Transversalis fascia hernioplasty.
N.Y. State J. Med. 80: 25-27, 1980
GLASSOW F.: The surgical repair of inguinal and femoral
hernias. Can. Med. Assoc. J. 108: 308-313, 1973
GRIFFIT C.A.: The Marcy repair of indirect inguinal hernia.
In: NYHUS L.M., CONDON R.E. (eds): Hernia. Edition 2. J.B. Lippincott Co.
Philadelphia, 1978
HALVERSON K. McVAY C.B.: Inguinal and femoral hernioplasty.
A 22 years study of the author's methods. Arch. Surg. 101: 127-135, 1970
ILES J.D.H.: Specialization in elective herniorrhaphy
Lancet 1: 751-755, 1965
Mc VAY C.B.: Inguinal and femoral hernioplasty: Anatomic
repair. Arch. Surg 57: 524-530, 1948
TONS C. et al.: Cremaster resection in Shouldice repair.
A prospective controlled bicenter study. Chirurg. 61(2): 109-111, 1990
5
MESH REPAIR
INDEX
Mesh repair is not a feature of traditional methods, because
the materials available before polypropylene were inappropriate. From the
beginning of the 20th century, numerous techniques using metal
mesh or tissue-implants were devised to solve the problem of defects in
large hernias, but the results were unacceptable.
At the end of the 1950's, meshes made of plastic and
well tolerated by the tissues, were introduced. Preperitoneal approaches
flourished again and particular attention was paid to traditional methods,
which were then improved. New techniques which made meshes a focal feature,
even in the treatment of primary hernias, were devised. According to those
who advocate meshes, these should be used in all cases, because they avoid
suture tension completely and reduce the incidence of recurrence considerably.
Today, the most frequently used meshes are those made
of polypropylene, Dacron and PTFE.
Current techniques position meshes in the preperitoneum
or between the intermediate layer (internal oblique muscle and aponeurosis
of the transversus) and the external oblique aponeurosis.
As in traditional methods, the approach may be inguinal,
preperitoneal or laparoscopic.
Only the most widely performed techniques will be discussed
here.
The Rives technique
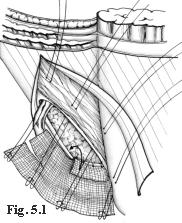
 This
technique was created in 1965. The approach is inguinal. The cremaster
is sectioned near the deep ring. The transversalis fascia is cut along
the inguinal canal, so that the Cooper ligament is exposed. A preshaped
(10 x10 cm) mesh of Dacron with a curved lacuna for the passage of the
iliac vessels, is fixed onto the Cooper ligament using 4-5 stitches along
the approximately 3-cm hem of the inferior flap. The flap is positioned
behind the iliopubic branch to increase the contact surface. The medial
flap of the mesh is fixed on the deep surface of the wide muscles by means
of a series of U-shaped stitches that penetrate the intermediate layer.
A cut is performed on the superoexternal side of the mesh as far as the
deep ring layer to allow for the passage of the funiculus (Fig. 5.1). The
flaps of the mesh are sutured to the wall using more U-shaped stitches,
to form a ring, positioned as high up as possible and calibrated around
the funiculus. At its inferior-external border the mesh is sutured to the
vascular sheath and to the inguinal ligament. Then the surplus mesh is
removed along the superoexternal side. The transversalis fascia is sutured
onto the prosthesis (Fig. 5.2). The funiculus is repositioned and the external
oblique aponeurosis sutured.
This
technique was created in 1965. The approach is inguinal. The cremaster
is sectioned near the deep ring. The transversalis fascia is cut along
the inguinal canal, so that the Cooper ligament is exposed. A preshaped
(10 x10 cm) mesh of Dacron with a curved lacuna for the passage of the
iliac vessels, is fixed onto the Cooper ligament using 4-5 stitches along
the approximately 3-cm hem of the inferior flap. The flap is positioned
behind the iliopubic branch to increase the contact surface. The medial
flap of the mesh is fixed on the deep surface of the wide muscles by means
of a series of U-shaped stitches that penetrate the intermediate layer.
A cut is performed on the superoexternal side of the mesh as far as the
deep ring layer to allow for the passage of the funiculus (Fig. 5.1). The
flaps of the mesh are sutured to the wall using more U-shaped stitches,
to form a ring, positioned as high up as possible and calibrated around
the funiculus. At its inferior-external border the mesh is sutured to the
vascular sheath and to the inguinal ligament. Then the surplus mesh is
removed along the superoexternal side. The transversalis fascia is sutured
onto the prosthesis (Fig. 5.2). The funiculus is repositioned and the external
oblique aponeurosis sutured.
The principles of this technique
The principles of this technique are complete treatment
of the myopectineal orifice and substitution of the transversalis fascia
with strong material.
Comments
The advantage of this technique is that it requires neither
a large mesh nor major dissections, while anchorage of the mesh to the
Cooper ligament is strong. The physiology of the inguinal canal is respected.
The author, who, while using this technique witnessed
a 0.6% recurrence rate, recommends it in cases of direct mediumdefect
and recurrent hernias. I sincerely retain this technique to be efficient.
My only doubts concern the U-shaped stitches that may cut through tissues
and open up new hernial defects.
Modern laparoscopic surgery, even if it accedes though
other approaches, uses a mesh anchored to the Cooper ligament and to the
wall and achieves repairs similar to those obtained by the Rives technique.
Lichtensteins "tension-free" hernioplasty
The approach is inguinal. Respect of the iliohypogastric,
ilioinguinal and genital branch of the genitofemoral nerves is recommended.
To respect the latter the author recommends isolating it with the funiculus
and dividing the cremaster at the level of the internal ring, avoiding
to cut the nerve. The hernial sac is bent inwards without ties. The external
oblique aponeurosis is separated from the level below on which a mesh of
polypropylene is positioned. An 8 x 16cm spindle shaped mesh is cut to
fit the inguinal area.
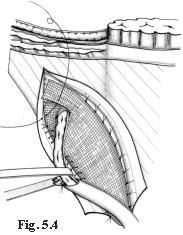
The procedure starts at the inferior-medial angle: the
mesh has to cover completely and exceed the pubic spine, then, it is sutured
on the fascial tissue, which covers and surrounds the bone without including
the periosteum. This suture runs between the margin of the mesh and the
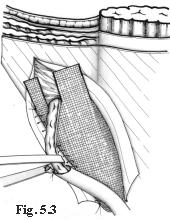
inguinal canal to the deep ring level. The border of the superolateral
mesh is cut to create two flaps: a wider superomedial one (2/3) and a narrower
inferior-lateral one (1/3) (Fig. 5-3). The superomedial flap is passed
below the spermatic cord and directed cranially. The mesh is stretched
under the funiculus and at the level of the deep ring, which is located
between two flaps.
The medial margin of the mesh is sutured onto the rectus
sheath, the superomedial one is put over the inferior lateral one, to circumscribe
the funiculus. The two flaps, overlapping one another, are sutured together
with one stitch at the inguinal ligament, immediately above the deep ring
(Fig.5-4).
Then, the mesh is cut to eliminate the surplus, 3-4 cm
above the deep ring. The external oblique aponeurosis is sutured.
Principles of the technique
The author, a strong supporter of prostheses (polypropylene
and monofilament), trusts in the findings of many studies regarding metabolic
collagen disorders in adults affected by hernia and speaks of the low trustworthiness
of tissues lacking in collagen fiber. He also believes that suture tension
should be avoided.
Comments
Much can be said about the lack of collagen. This may
be due to a reduction in solicitation of the aponeurosis resulting from
muscular weakening. Less strength means less solicitation. Moreover, the
excellent results obtained by the Shouldice technique disprove the theory
that "collagenlow" tissue is unreliable.
As regards the so-called "tension free" techniques (an
intriguing and exciting slogan) I would like to make two observations:
- the absence of tension occurs only at rest, with very
slight endoabdominal pressure and a loosened wall. But in the erect position
and under strain, tension spreads uniformly to the whole abdominal wall.
- On a non-contractile surface (passive area) the push
of the endoabdominal pressure causes what I call the "sail effect" and
determines traction on the perimeter of the passive zone proportional to
the surface itself.
There are still doubts regarding the position of the
mesh on top of the internal oblique muscle. The posterior wall is, indeed,
reinforced by the mesh, but it is not "sealed". There is a definite risk
of intramural hernias, even if they are small and clinically irrelevant.
Concluding, physiology is not respected because the neo- deep ring, made
of mesh, is anchored to the inguinal ligament and the internal oblique
muscle is entangled in the scar tissue.
Despite these disputable aspects, the technique produces
good results. The author shows a 0.1% recurrence and points out that specific
experience is not required to obtain good results.
The sutureless "Mesh-Plug" technique

 The
approach is inguinal.
The
approach is inguinal.
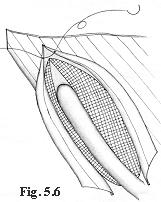
In indirect hernias, Gilbert uses a plug consisting in
a (5 x 5 cm) polypropylene square, on which a cut, from the middle of one
side to the center, is made. The plug is folded many times, as shown on
Figure 5.5, assuming a roughly triangular shape. It is then inserted into
the hernial defect and abandoned. According to the author the plug expands
completely inside the preperitoneum creating a posterior barrier. A second
polypropylene sheet (5 x 9 cm), is shaped to fit and positioned on top
of the transversalis fascia and internal oblique muscle. A cut is made
on the superolateral margin to allow the funiculus to pass. No stitches
are used. The mesh remains in place while the external oblique aponeurosis
is sutured in front of it (Fig. 5.6).
The Gilbert technique has inspired many more which differ
only in as far as the type of plug and the shape of the mesh positioned
in front of the transversalis fascia and internal oblique muscle, are concerned.
Robbins and Rutkow suggest other types of plug (conical
or preshaped) and perform this technique on all hernias. When the hernial
defect is large, a bigger plug is used and is sutured to the edges of the
hernial defect to avoid dislocation.
Principles of the technique
Simplicity, rapidity and minimized dissection characterize
this technique. According to Gilbert, stitches through the transversalis
fascia used to calibrate the deep ring , may distort and weaken the fascia
itself, leading to recurrence.
Comments
The most important feature of this technique is its minimization
of dissection. No sutures occur to weaken the tissues around the "critical
zone", that is, the edge of the mesh. Usually this is where greatest solicitation
occurs, as shown by the site of recurrences.
It is not true that inexperienced surgeons are in a position
to avail of this technique. Hernia treatment requires, in all cases, skill
and experience because, however easy an operation may appear at first sight,
it may present sudden and expected difficulties. Repair is not necessarily
the most complicated phase of a hernia operation.
Furthermore I disagree with the use of exceedingly large
quantities of mesh as required to make plugs.
The method is presented as physiological and it is in
part. However, the mesh positioned in front of the transversalis fascia,
provokes a scar reaction capable of entangling the internal oblique muscle,
even in the absence of sutures.
The Stoppa technique (with giant extraperitoneal mesh)
Stoppa elaborated this technique on the basis of a previous
study by Mahorner and Goss (1962), eliminating the stitches used to anchor
the mesh to the wall.
The approach is preperitoneal through a midline umbilical
pubic incision. A wide cleavage in the preperitoneal area is performed,
involving the space from the Retzius and bladder to the prostate, reaching
laterally beyond the inferior epigastric vessels and below the rectus muscle
to the inguinal region. Once the hernial sac is reached, it is isolated
by means of moderate traction. If adhesions occur they should be carefully
dissected by introducing a finger into the sac itself. Once the sac is
freed, separation continues downwards to the iliac vessels and laterally
to the iliac psoas muscle. Then the testicular vessels are separated them
as much as possible from the peritoneum, so that they adhere to the wall
and do not cross the preperitoneal space where the mesh will be positioned.
At this stage the surgeon should stand on the side facing the area to be
detached, although during the rest of the operation he/she stands on the
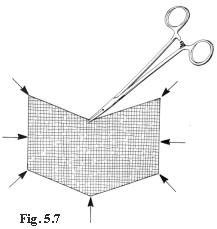
other side. As soon as the separation has been carried out, a mesh of Dacron
is prepared. It should be tailored to fit the patient and correspond transversally
to 2 cm less than the distance between the anterior-superior iliac spines
(about 26 cm) and vertically to the distance between the umbilicus and
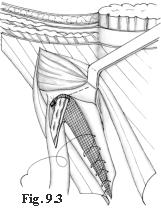
pubis (roughly 16 cm). A very wide V shape 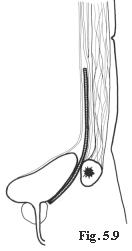 is
cut into the top and bottom of the mesh (Fig.5.7). Then 8 Rochester forceps
are positioned at the angles and
is
cut into the top and bottom of the mesh (Fig.5.7). Then 8 Rochester forceps
are positioned at the angles and
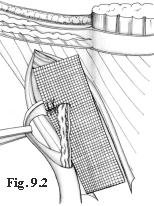
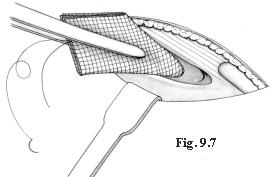
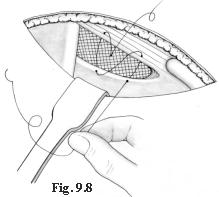
in the midpoints of each side of the mesh. The preperitoneal
area is opened wide and the mesh positioned (Figs. 5.8, 5.9) using the
Rochester forceps. The central lower border forceps is inserted between
the pubis and bladder, followed by the inferolateral forceps, then those 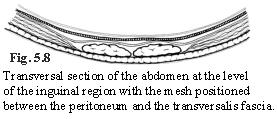 positioned
at the midpoint of the lateral margin and, lastly, those at the superolateral
angle. The forceps are then pushed as far apart as possible in order to
unfold the mesh. They are then removed with great care to avoid dislocating
the mesh. The same sequence is performed on the other side. Again, the
surgeon will stand on the side opposite the area to be treated. The mesh
is fixed to the wall with one stitch passing through the upper marginal
midpoint. The laparotomic wound is then sutured.
positioned
at the midpoint of the lateral margin and, lastly, those at the superolateral
angle. The forceps are then pushed as far apart as possible in order to
unfold the mesh. They are then removed with great care to avoid dislocating
the mesh. The same sequence is performed on the other side. Again, the
surgeon will stand on the side opposite the area to be treated. The mesh
is fixed to the wall with one stitch passing through the upper marginal
midpoint. The laparotomic wound is then sutured.
Principles of the technique
The giant mesh has the task of surrounding the visceral
sac and reinforcing the transversalis fascia bilaterally in particular
at Fruchaud myopectineal orifice level. The mesh is not anchored by stitches,
because it reaches beyond the hernial defect. According to Pascal's hydrostatic
principle, it is pushed against the wall by internal-abdominal pressure.
This pressure is proportional to the surface of the mesh and blocks the
movement.
Comments
This technique respects physiology. The positioning of
the testicular vessels along the wall avoids creating gaps in the mesh,
a constant source of critical weakness.
It should be underlined that: 1) the amount of foreign
body introduced is considerable. 2) the separation area is so wide that
this technique cannot possibly be performed in local anesthetic. 3) this
kind of surgery requires training. 4) the indications provided are not
many: plurirecurrent hernias, very large hernias, and bilateral hernias.
It is, in any case, a very interesting technique and performed by the author,
shows a recurrence rate of 0.56%.
The Wantz preperitoneal technique
This is a variation of the Stoppa technique.
Wantz uses a mesh corresponding to 1 cm less than the
distance between the midline and the anterior-superior iliac spine. The
depth of the mesh depends on the patient's body size, usually between 12
and 14 cm. The mesh is inserted (in local anaesthetic) through a transversal
lateral incision. The transversalis fascia is cut longitudinally, near
the border of the rectus muscle. A large mesh is introduced into the preperitoneum
and sutured to the wall where more accessible, but at deeper-seated level
the mesh is positioned between peritoneum and wall without suture. The
mesh may be fenestrated to permit the passage of the testicular vessels
or may be positioned above them, once they have been isolated from the
peritoneum for a considerable distance.
The Nyhus technique
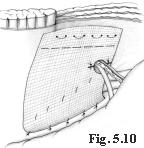
Thanks to Nyhus, the preperitoneal approach was relaunched
in 1959. He proposes a suprainguinal approach and suture of the hernial
defect from within. In hernia recurrences, he uses a mesh to reinforce
the suture of the hernial defect. He uses a cm 6 x 14 rectangle in polypropylene.
He fixes it with unabsorbable stitches to the Cooper ligament and to the
posterior suture of the hernia defect. He positions it and fixes it with
U-shaped stitches behind the operating wound, to protect it (Fig. 5-10).
Laparoscopic hernioplasty
E. Nicolo'
The transabdominal, preperitoneal and completely extraperitoneal
approaches have already been amply illustrated in chapter 2. The reader
should therefore refer back to what has already been said for data regarding
the initial phases of this technique.
The transabdominal preperitoneal approach
While the peritoneum is still intact, using hand pressure
on the outside of the abdominal wall, the pubic spine corresponding to
the midline is identified.
The first structure identified is the umbilicus-lateral
bladder ligament (the medial border for the dissection of the peritoneum).
This ligament may be divided using clips to obtain a
better vision of the medial portion of the inguinal region. The bladder
should also be identified so as to avoid damage to it.
Moving down along the umbilicus-lateral bladder ligament,
we find the deferent canal which, stemming from the pelvis, follows a medial-lateral
path in the direction of the deep inguinal ring.
At this level the deferent canal joins the internal spermatic
vessels, which follow a lateral-medial path and form an upturned V shape.
The highest point of this V corresponds to the deep inguinal ring and is
directed upwards as if pointing to the inferior epigastric vessels.
The inferior epigastric vessels are not always easily
identifiable, especially in obese patients, even when the peritoneum is
intact.
The parietal peritoneum is cut as high as possible (Fig.
5.11) 2-3 cm from the lateral border of the deep inguinal ring medially
to the umbilicus-lateral bladder ligament.
Cap
2
 First,
the upper peritoneal flap is dissected smoothly. The lower peritoneal flap
is treated in the same way up to iliac vessel level.
First,
the upper peritoneal flap is dissected smoothly. The lower peritoneal flap
is treated in the same way up to iliac vessel level.
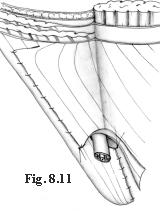
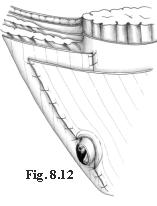
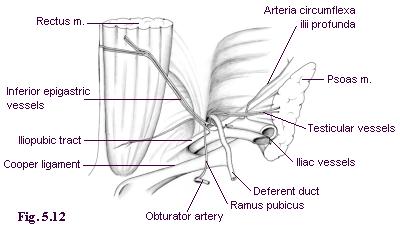
The lower epigastric vessels if not identifiable while
the peritoneum is intact, will be when it is opened (Fig. 5.12). During
the preparation of the flaps, particular attention should be paid to the
peritoneal vessels. The aponeurosis of the transversus muscle is identified
above the deep inguinal ring. It is then followed medially to its insertion
with the Cooper ligament, close to the pubic spine.
The iliopubic tract (or Thompson ligament) is identified
at the lower edge of the deep inguinal ring. It lies parallel to the inguinal
ligament, is situated closer to the surface and is not laparoscopically
visible.
Following the iliopubic tract medially, the Cooper ligament
is then identified. The circumflexa ilii profunda artery is easily identified,
because it is parallel to the iliopubic tract.
In indirect hernia, the sac must be carefully isolated
from the spermatic cord and introflexed. When the sac is too large it may
be resected, as occurs in the presence of an adipocele.
In femoral hernia the Cooper and Thompson lacunar ligaments
are exposed. The deferent canal and internal spermatic vessels are isolated
smoothly, creating a gap between these elements and the iliac vessels.
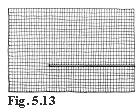
A Prolene mesh of 7.5 x 12 cm is cut as illustrated in
Figure 5.13 (a cut parallel to the longer side and about 2/3 its length
is performed at about 1/3 from the bottom of the shorter side).
The mesh, having been rolled, is introduced into the
abdominal cavity. Using a trocar and a dissector it is positioned so that
the small flap passes through the opening previously used by the iliac
vessels and deferent canal.
The large flap is used to cover the inguinal ring.
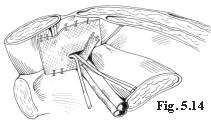
The mesh is fixed, using clips, first onto the Cooper
ligament then onto the abdomen wall to the right and the left of the epigastric
vessels. Finally, both borders of the mesh are joined and fixed by clips
above the iliopubic tract (Fig. 5.14).
The clips should be inserted above the iliopubic tract
to avoid lesion of the iliac vessels and of the nerves immediately beneath
this structure.
Clips or continuous stitching suture both peritoneal
borders. The trocars are moved under direct surveillance and the pneumoperitoneum
is reduced. The skin incisions are closed by intradermic suture.
In cases of inguinal-femoral hernia in women the mesh
is not cut as indicated above but positioned whole and fixed at the same
levels above the round ligament.
The preperitoneal approach
Once the preperitoneal region has been reached, as described
in chapter 2, the same situation as in the transperitoneal approach presents
itself once the peritoneum has been opened.
The operating step is similar to that described in the
preperitoneal transabdominal approach. The only difference is that no repair
of the peritoneum occurs.
INDEX
References.
AJABNOOR M.A., MOKHTAR A.M., RAFEE A.A., TAHA A.M.: Defective
collagen metabolism in Saudi patients with hernia. Ann. Clin. Biochem.
29 (4): 430-436, 1992.
AMID P.K., SHULMAN A.G., LICHTENSTEIN I.L.: Critical
scrutiny of the open "tension-free" hernioplasty. Am. J. Surg. 165: 369-371,
1993.
AMID P.K., SHULMAN A.G., LICHTENSTEIN I.L.: Femoral hernia
resulting from inguinal herniorrhaphy: the "plug" repair. Cont. Surg. 39:
19-24, 1991.
ARNAUD J.P., ELOY R., ADLOFF M., GRENIER J.F.: Critical
evaluation of prosthetic materials in repair of abdominal wall hernias.
New criteria of tolerance and resistance. Am. J. Surg. 133: 338-345, 1977.
ARNAUD J.P., ELOY R., WEILLBOUSSON M., GRENIER J.F.,
ADLOFF M.: Résistance et tolérance biologique de 6 prothèses
utilisées dans la réparation de la paroi abdominale. J. Chir.
113: 85, 1982.
BARNES J.P.: Inguinal hernia repair with routine use
of Marlex mesh. Surg. Gynecol. Obstet. 165: 33-37, 1987.
CAPOZZI J.A., BERKENFIELD J.A., CHEATY J.K.: Repair of
inguinal hernia in the adult with Prolene mesh. Surg. Gynecol. Obstet.
167: 124-128, 1988.
CHEATLE G.L.: An operation for the radical cure of inguinal
and femoral hernias. Br. Med. J. 2: 68, 1920.
CONDON R.E.: The anatomy of the inguinal region. In:
NYHUS L.M., HARKINS H.N. (eds.): Hernia. ed 2., J.B. Lippincott, Philadelphia,
1964, p. 14.
CORBITT J.D.: Laparoscopic herniorrhaphy. Surg Laparosc
Endosc 1991; 1:23-25.
FILIPI C.J., FITZGIBBONS R.J., SALERNO G.M., HART R.O.:
Laparoscopic herniorrhaphy. In: Laparoscopy for the General Surgeon. Surg.
Clin. North Am., 1992.
FITZGIBBONS R.J., SALERNO G.M., FILIPI C.J., HUNTER W.J.:
A laparoscopic intraperitoneal onlay mesh technique for the repair of an
indirect inguinal hernia. Ann Surg 1994; 219(2):144-156.
FITZGIBBONS R.J.: Laparoscopic inguinal hernia repair.
Paper presented at New Frontiers in Endoscopy Nationwide Satellite Teleconference.
1991 (May 15).
FRUCHAUD H.: Anatomie chirurgicale des hernies de l'aine.
Doin, Paris, 1957.
GATT M.T., CHEVREL J.P.: The treatment of neuralgia following
inguinal herniorrhaphy: a report of 47 cases. Postgrad. Gen. Surg. 4 (2):
142-147, 1992.
GILBERT A.I.: An anatomical and functional classification
for the diagnosis and treatment of inguinal hernia. Am. J. Surg. 157:331-333,
1989
GILBERT A.I.: Inguinal hernia repair. Biomaterials and
sutureless repair. Perspectives in Gen. Surg. Vol. 2, 1: 113-129, 1991.
GILBERT A.I.: Sutureless repair of inguinal hernia. Am.
J. Surg. 163:331-335, 1992
HALSTED W. S.: The radical cure of inguinal hernia in
the male. Bull. of the Johns Hopkins Hospital IV, 29: 17, 1893.
HARRISON P.W.: Inguinal hernia. A study of the principles
involved in surgical treatment. Arch. Surg. 4: 680, 1922.
HAWASLI A.: Laparoscopic inguinal herniorrhaphy: Classification
and 1 year experience. J. Laparoendoscopic Surgery, 1992.
HENRY A.K.: Operation for femoral hernia by a midline
extra peritoneal approach. Lancet 19: 531-533, 1936.
KAVIC M.S.: Laparoscopic hernia repair. Surg. Endosc
1993; 7:163-167
KAVIC MS.: Laparoscopic hernia repair. Harwood Academic
Publishers Amsterdam 1997
LICHTENSTEIN I.L., SHORE J.M.: Simplified repair of femoral
and recurrent inguinal hernias by a "plug" technique. Am. J. Surg. 128:439-444,
1974
LICHTENSTEIN I.L., SHULMAN A.G., AMID P.K., MONTLLOR
M.: Cause and prevention of post-herniorrhaphy neuralgia: a proposed protocol
for treatment. Am. J. Surg. 155: 786-790, 1988.
LICHTENSTEIN I.L., SHULMAN A.G., AMID P.K.I. et al: The
tension-free hernioplasty. Am. J. Surg. 157:188-193, 1989
LICHTENSTEIN I.L., SHULMAN A.G.: Ambulatory outpatient
hernia surgery, including a new concept, introducing tension-free repair.
Int. Surg. 71:1-7, 1986
MAHORNER H., GOSS G.M.: Herniation following destruction
of Poupart's and Cooper's ligaments: a method of repair. Ann. Surg. 155:
741-747, 1962.
McKERNAN J.B., LAWS H.L. : Laparoscopic repair of inguinal
hernias using a totally extraperitoneal prosthetic approach. Surg. Endosc.
1993; 7:26-28.
NOLEN M., MELICHAR R., JENNINGS W.C., McGEE M.C.: Use
of a Marlex fan in the repair of direct and indirect Hernias by laparoscopy.
Laparoendoscopic Surg., 1992.
NYHUS L.M. et al.: The preperitoneal approach and prosthetic
buttress repair for recurrent hernia: the evolution of a technique. Ann.
Surg. 208: 733-737, 1988.
NYHUS L.M., CONDON R.E., HARKINS H.N.: Clinical experiences
with preperitoneal hernia repair for all types of hernias of the groin.
Am. J. Surg. 100: 234, 1960.
NYHUS L.M.: Inguinal hernia. Curr. Prob. Surg. XXVIII-6:
406-450, 1991.
PEACOCK J.R. E.E.: Wound repair. 3rd Ed, WB Saunders
Co., Philadelphia, 1984, pp. 336-337.
PEACOCK E.E.: Here we are again: behind again! Am. J.
Surg. 157: 187, 1989.
QUILICI P.J.: New Developments in Laparoscopy. CT: USS
P. Press, Norwalk, 1992.
READ R.C.: A review: the role of protease-antiprotease
imbalance in the pathogenesis of herniation and abdominal aortic aneurysm
in certain smokers. Post. Gen. Surg. 4 (2): 161-165, 1992.
RIVES J. FLAMENT J.B., DELATTRE J. F., PALOT J. P.: Traitement
des hernies de l'aine à l'aide de prothèses mises en place
par voie inguinale directe. Travaux du GREPA, Ed. Bruneau 5: 18-24, 1983.
RIVES J., FLAMENT J.B., DELATTRE J.F., PALOT J.P.: La
chirurgie moderne des hernies de l'aine. Cah. Med. 7: 1205-1218, 1982.
RIVES J., FORTESA L., DROUARD F., HIBON J., FLAMENT J.B.:
La voie d'abord abdominale sous-péritonéale dans le traitement
des hernies de l'aine. Ann. Chir. 32: 245-255, 1978.
RIVES J., LARDENNOIS B., FLAMENT J.B., CONVERS G.: La
pièce en tulle de Dacron, traitement de choix des hernies de l'aine
de l'adulte, à propos de 183 cas. Chirurgie 99: 564-575, 1973.
RIVES J., LARDENNOIS B., FLAMENT J.B., HIBON J.: Utilisation
d'une étoffe de Dacron dans le traitement des hernies de l'aine.
Acta Chir. Bel. 70: 284-286, 1971.
RIVES J., LARDENNOIS B., HIBON J.: Traitement moderne
des hernies de l'aine et de leurs récidives. Encyclopédie
Med. Chir. Techniques Chirurgicales 1 (40 110): 1-12, 1973.
RIVES J., NICAISE H., LARDENNOIS B.: A propos du traitement
chirurgical des hernies de l'aine. Orientation nouvelle et perspectives
thérapeutiques. Ann. Med. Reims 2: 193-200, 1965.
RIVES J., NICAISE H.: A propos des hernies de l'aine
et de leurs récidives. Sem. Hòp. 31: 1932-1934, 1966.
RIVES J., STOPPA R., FORTESA L., NICAISE H.: Les pièces
en tulle de Dacron et leur place dans la chirurgie des hernies de l'aine.
Ann. Chir. 22: 159-171, 1968.
RIVES J.: Surgical treatment of the inguinal hernia with
Dacron patch. Int. Chir. 47: 17) 360-361, 1967.
ROBBINS A.W., RUTKOW I.M: The Mesh-plug hernioplasty.
Surg. Clin. NA. 73: 501-512,1993
SCHULTZ L., GRABER J., PIETRAFITTA J., HICKOK D.: Laser
laparoscopic herniorrhaphy: A clinical trial, preliminary results. J. Laparoendoscopic
Surg. 1: 41-45, 1990.
SHULMAN A.G., AMID P.K., LICHTENSTEIN I.L.: Prosthetic
mesh plug repair of femoral and recurrent inguinal hernias: the American
experience. Ann. Royal Coll. Surg. Engl. 74: 97-99, 1992.
SHULMAN A.G., AMID P.K., LICHTENSTEIN I.L.: The safety
of mesh repair for primary inguinal hernias: results of 3,019 operations
from five diverse surgical sources. Am. Surg. 58: 255-257, 1992.
STARLING J.R., HARMS B.A.: Diagnosis and treatment of
genitofemoral and ilioinguinal neuralgia. World J. Surg 13:586-591, 1989
STOPPA R., PETIT J., ABOURACHID: Procédé
original de plastie des hernies de l'aine. L'interposition sans fixation
d'une prothèse en tulle de Dacron par voie médiane prépéritonéale.
Chirurgie 99: 119, 1973.
STOPPA R.E., RIVES J.L., WARLAUMONT C.R. et al: The use
of Dacron in the repair of hernias of the groin. Surg. Clinic. North Am.
64: 269, 1984.
STOPPA R.E., WARLAUMONT C.R.: The midline preperitoneal
approach and the prosthetic repair of groin hernia. In: NYHUS L.M., BAKER
R.J. (eds.): Mastery of Surgery. 2nd ed., Little Brown Ed., Boston, 1992.
STOPPA R.E., WARLAUMONT C.R.: The preperitoneal approach
and prosthetic repair of groin hernia. In: NYHUS L.M., CONDON R.E. (eds.):
Hernia. 3d ed, J.B. Lippincott, Philadelphia e Toronto, 1 vol., 1989.
USHER F.C., ALLEN J.E., CROSTHWAIT R.W., COGAN J.E.:
Polypropylene monofilament. A new, biologically inert suture for closing
contaminated wounds. JAMA 179: 780, 1962.
WAGH P.V., LEVERICH A.P., SUN C.N., WHITE H.J., READ
R.C.: Direct inguinal herniation in men: a disease of collagen. J. Surg.
Res. 17: 425, 1974.
WANTZ G.E.: Atlas of Hernia Surgery. 1 vol. Raven Press
Ed., New York, 1991.
WANTZ G.E.: Giant reinforcement of the visceral sac.
Surg. Gynceol. Obstet. 169: 408, 1989.
WILLIS I.H., SENDZISCHEW H.: Laparoscopic pre-peritoneal
prosthetic inguinal herniorrhaphy. Laparoendoscopic Surg., 1992.
PART TWO
PHYSIOLOGICAL HERNIOPLASTY
6
A REEXAMINATION
OF THE INGUINAL REGION FROM AN ANATOMICAL AND FUNCTIONAL POINT OF VIEW
INDEX
The inguinal region has been studied thoroughly. However,
I think that some important anatomical and physiological aspects should
be given greater consideration. Therefore, I should like to highlight these
aspects in order to discuss the theoretical premises of the physiological
hernioplastic method.
The anatomical and functional aspects of the anterior abdominal wall
The anterior abdominal wall is composed of muscles, fascias
and aponeuroses. The fascias cover the muscles. The aponeuroses are flat
tendons, anatomical continuations of the corresponding muscles characterized
by the collagen fibers aligned with those of the muscles.
The aponeuroses are considerably resistant to traction
in the direction of the fibers. When traction occurs in a transversal direction
the aponeuroses are not so resistant but are elastic.
The muscles and fascias are located in such a way as
to form a synergic system: at rest the fascias contain and protect
the muscles while under strain the muscles protect the fascias, because
as they contract they become very rigid.
The posterior wall of the inguinal canal and the linea
alba are the only areas not sustained by muscles in the anterior abdominal
wall. In normal conditions these are very narrow. We use the expression
passivearea to indicate an area of the abdominal wall consisting
only of fascia, but no muscle, because it does not react actively to the
increase in internal pressure caused by the prelum abdominale.
When the abdominal muscles contract:
- the muscles harden and shorten
- the diameters of the abdominal cavity are reduced
- the fascial zones, protected by the muscles, and not
subject to stress, relax
- the aponeuroses are placed under tension in the direction
of their fibers
- the endoabdominal pressure increases considerably
- the fascial zones which are not protected by muscles
(passive areas) receive a solicitation from an endoabdominal pressure
proportionate to the dimension and to the bend radius of their surfaces.
To clarify this last statement, it is necessary to consider
the effects of the endoabdominal pressure on a passive area according to
Laplace's law.
Laplace's law applies to elastic cylindrical
or spherical containers, which undergo an internal pressure greater than
the external one: the relationship between the transmural pressure (P),
the tension of the wall in a point (T) and the bend radius (r) of the wall
in that point is T= P x r in a cylindrical container, T= P x r/2 in a spherical
container.
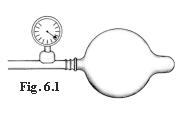
More simply, the tension caused by a constant internal
pressure upon each point of the wall, in an elastic cylindrical or spherical
container, is proportional to the bend radius at that point. For
example, when a cylindrical balloon is inflated, the proximal tract inflates
first and this increases the length of its radius.
As the air enters, the proximal tract inflates while
the distal tract, which has a shorter radius, does not and is less stressed
even though it is subject to the same pressure (Fig. 6.1). It is surprising
to observe how soft the wall of the undilated tract is and how little resistance
it opposes, in contrast with the obvious tension and hardness of the dilated
tract.
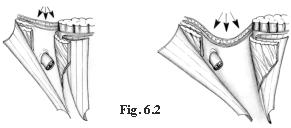 Due
to the effect of the prelum abdominale, the passive area, not being
contractile, neither reduces its dimensions nor increases its consistency.
This is therefore subject to the thrust caused by endoabdominal pressure
and assumes a shape comparable to a concave spherical or cylindrical segment,
proportionate to the length of its principle axes (Fig. 6.2). If a passive
area is narrow, though long, it will undergo very little stress
produced by endoabdominal pressure, because under strain it will assume
the shape of a cylindrical segment with a short radius.
Due
to the effect of the prelum abdominale, the passive area, not being
contractile, neither reduces its dimensions nor increases its consistency.
This is therefore subject to the thrust caused by endoabdominal pressure
and assumes a shape comparable to a concave spherical or cylindrical segment,
proportionate to the length of its principle axes (Fig. 6.2). If a passive
area is narrow, though long, it will undergo very little stress
produced by endoabdominal pressure, because under strain it will assume
the shape of a cylindrical segment with a short radius.
The structural aspects of the main anatomic layers of the inguinal
region in normal conditions and in hernia patients
In males, the inguinal region represents a critical area
due to a number of peculiar characteristics:
-
the inguinal canal is weak because the spermatic cord which
is soft, mobile and opposes no resistance to stress, passes through it
-
there is more presence of fascial and aponeurotic tissue
and little muscle presence
-
the deep and superficial rings represent two weak points.
The posterior layer
The posterior layer of the inguinal region consists of
the transversalis fascia and of the transversus muscle with its aponeurosis.
The deep ring is located at this level.
The transversus muscle is not so well represented and
borders on the superoexternal side of the deep ring; its aponeurosis borders
on the inferior-medial side of the deep ring.
The passive area corresponding to the posterior wall
of the inguinal canal is formed by the transversalis fascia and by the
iliopubic tract. This area is not very strong but is very narrow. Medially
the aponeurotic arch of the transversus muscle adheres to the transversalis
fascia, covered by the internal oblique muscle and is characterized by
curved and rather thin fibers.
Often in hernia patients, the posterior wall of the inguinal
canal is wide and thin. In the indirect hernia the deep ring is quite wide,
surrounded by weak tissues with adipocele on the lateral side. The transversalis
fascia is very thin and often unrecognizable from the external side of
the deep ring.
The intermediate layer
 The
intermediate layer consists in the spermatic cord and the internal oblique
muscle. The spermatic cord is soft and therefore alters the synergy existing
between the anatomical planes. The internal oblique muscle with its free
margin surrounds the funiculus at the exit of the deep ring; then, it continues
along the funiculus as far as the pubis. In this way, it forms the whole
medial margin of the inguinal canal. The distance between the internal
oblique muscle and the inguinal ligament is minimal.
The
intermediate layer consists in the spermatic cord and the internal oblique
muscle. The spermatic cord is soft and therefore alters the synergy existing
between the anatomical planes. The internal oblique muscle with its free
margin surrounds the funiculus at the exit of the deep ring; then, it continues
along the funiculus as far as the pubis. In this way, it forms the whole
medial margin of the inguinal canal. The distance between the internal
oblique muscle and the inguinal ligament is minimal.
In hernia patients (except for some congenital hernias
affecting young people), the lower margin of the internal oblique muscle
seldom reaches the pubis. Its inferior fibers reach the rectus sheath at
a variable distance from the pubis, even 3-4 cm. Therefore, a passive area,
the inguinal triangle (Fig. 6.3) is formed. This triangle has not
to be confused with the triangle of Hesselbach. Bordering on this inguinal
triangle are the internal oblique muscle, the rectus sheath and the inguinal
ligament. Very often the internal oblique muscle is hypotrophic.
Cap 1 Cap 11
The superficial layer
The superficial layer is represented by the external
oblique aponeurosis which is characterized by its oblique-oriented fibers.
In hernia patients, the external oblique aponeurosis
may be fiberdeficient or hypotrophic at the level of the superficial
ring, but usually it does not present large lesions, because the fibers
are longitudinally resistant and transversally elastic, and, unless the
hernia is very vast, does not lead to relevant damage.
The normal defense mechanisms of the inguinal region (sling, sphincter
and shutter mechanisms)
As an effect of the prelum abdominale, the aponeuroses
of the inguinal canal are subjected to two solicitations: one is the contraction
of the muscles and the other is an increase in endoabdominal pressure.
The former acts only in the direction of the fibers, while the latter acts
also transversally. The transversalis fascia is not stressed by the muscular
traction, but only by the endoabdominal pressure. As stated, the aponeuroses
do not resist much to traction along the transversal axis of the fibers.
Therefore, the solicitation which finds the inguinal canal in a position
of greater vulnerability is that provoked by endoabdominal pressure acting
in all directions.
The normal defense mechanisms of the inguinal canal protect
from the action of the prelum abdominale the two critical spots: the deep
ring, and the posterior wall of the inguinal canal represented by the only
transversalis fascia and by the iliopubic tract.
Protection of the deep ring
The contraction of the transversus muscle produces three
effects:
-it narrows the ring,
-it moves the ring in a lateral-cranial direction.
-it pulls it in a lateral-cranial direction of the superior
crus of the sling of the transversalis fascia.
As a consequence, the exceeding transversalis fascia
surrounding the deep ring closes on the deep ring itself like an eyelid
(sling effect).
At the same time, the internal oblique muscle contracts,
stiffens and lowers itself in front of the deep ring. This combined action
of the two muscles is called the sphincter effect.
Protection of the posterior wall of the inguinal canal
The simultaneous contraction of the transversus and the
internal oblique muscles creates the shutter mechanism: the aponeurotic
arch of the transversus stiffens, straightens and draws close to the iliopubic
tract. The same occurs for the arch formed by the internal oblique muscle.
In this way, the posterior wall of the inguinal canal
is at its narrowest and is barely stressed by the endoabdominal pressure,
according to Laplace's law.
The functional aspects of the inguinal region in hernia patients
In hernia patients, these defense mechanisms are seriously
altered.
The sling and sphincter mechanisms may be preserved in
direct hernia, but they may be severely altered in indirect hernia.
The shutter mechanism fails to occur at the inguinal
triangle, even if the internal oblique muscle contracts a lot. This
passive area may narrow, but it cannot be covered by the muscle.
When the internal oblique muscle is atrophic or so weak
as to fail to act as a defensive barrier, by contracting, it behaves as
a passive area. In this case, the fibers of the aponeurotic arch of the
transversus too will undergo solicitations transversally and will easily
dissociate.
Deductions
The posterior wall of the inguinal canal has a function
we have called sealing: a gap in the posterior level will certainly
determine the exit of a hernia, which cannot be stopped by the upper layers
We have many doubts about the emphasis placed on the
resistance of the transversalis fascia. It may be very resistant to solicitations
but only when the posterior wall of the inguinal canal is narrow and when
the protective action of the upper layers is efficacious.
There is no doubt that the inguinal region wall is a
synergic system where each of its levels has a specific role. In any case,
I have noticed that the posterior wall has been overestimated, while the
other two anatomic layers, even if indirectly involved in the formation
and development of a hernia, have been underestimated.
The other two anatomic layers are: the internal oblique
muscle, which is certainly the most important active defender of the inguinal
canal and the external oblique aponeurosis, which plays a very important
role in supporting the layers beneath.
I would like to underline the importance of the inguinal
triangle as a weak passive area. It is often wide and unprotected
by the shutter mechanism. Concluding, I would like to point out that narrowing
a passive area means reinforcing it.
According to what has been pointed out, the purposes
of a "functional" hernial therapy is:
- repair of the sealing function of the posterior
layer
- repair of the sphincter effect at the level of the
deep ring
- repair of the shutter mechanism.
Repair of the sealing function of the posterior layer
It is very important to separate the elements of the
funiculus from the proximal tract of the cremaster, in order to eliminate
even small adipoceles, because they stick to the cremaster and easily lead
to recurrences. A perfect calibration of the deep ring around the cord
elements is no less important. Anyway, one must consider that even after
a good repair has been performed, the poor quality of the tissues surrounding
the ring, make the risk of laceration greater.
Repair of the posterior wall of the inguinal canal is
fundamental in direct hernia. In this case, sometimes the stitches passing
through an entire wall may cut the tissues and open new hernial defects.
Repair of the sphincter effect at deep ring level
The action (narrowing and rising the deep ring so that
it be protected by the internal oblique muscle) of the transversus muscle
may be repaired as long as the deep ring remains on the same anatomical
level, free and independent of the levels above.
Repair of the shutter mechanism
In order to repair the shutter mechanism, the inguinal
canal must be narrowed and must border on the entire inferior-lateral
side of the internal oblique muscle. This means that if the lower lateral
margin of the internal oblique muscle is short and is inserted high on
the rectus sheath, the inguinal canal has to be short and end at the same
height.
The inguinal triangle has, therefore, to be excluded
from the inguinal canal. Like every other passive area, it has to be
reinforced and narrowed, compatibly with a moderate tension of the sutures.
These premises are necessary to explain the technical
choices of physiological hernioplasty. Its purpose is to repair the defense
mechanisms of the inguinal region respecting the principles of physics
and biology.
The myopectineal orifice
According to Fruchaud, the myopectineal orifice is bordered
on medially by the rectus sheath, superiorly by the transversus and internal
oblique muscles, laterally by the iliopsoas muscle, inferiorly by the pubis
covered by the Cooper ligament and by the pectineus muscle with its fascia.
Basically, this perspective believes that the two weak areas of the inguinal
and crural regions to be essentially one. The iliopubic tract and the inguinal
ligament, which cross and divide the myopectineal orifice, are considered
supporting elements of minor importance.
This position has been supported by those who advocate
suturing or better still insertion of meshes into the entire weak area
corresponding to the myopectineal orifice. Reality has belied this perspective:
crural hernia is far less frequent than inguinal hernia. Evidently, the
iliopubic tract and the inguinal ligament have a very important role as
"support beams", also because they occur in an angular area, so that, according
to Laplace's law, the stress is reduced due to the existence of a short
bend radius.
I believe it is better to limit the surgical trauma.
Too often supporters are overenthuiastic about the "the myopectineal
orifice" and this leads to the practice of ample dissections and applications
of meshes anchored to the Cooper ligament without any specific indication.
INDEX
7
WHY A NEW METHOD?
INDEX
Traditional methods tend to repair normal anatomy without
respecting the physiology of the area. It is well known that sutures under
tension or which pass through the whole wall can open new hernial defects,
create ischemia and impede perfect healing. Recurrences widely exceed the
10% mark in patients not treated in specific hernia units.
Meshes substitute and reinforce tissues, avoid suture
tension, but they do not eliminate passive areas. Physiology of the inguinal
region is hardly ever respected even in prosthetic surgery. With meshes,
recurrences are definitely reduced compared to traditional methods. But
even if mesh technique is expanding today, direct suture still remains
the most common.
Today, some prosthetic methods have a recurrence incidence
of close on 0%. Is there any possibility for further progress? Is there
any need for a "post mesh"?
I usually use mesh and think that in many cases it is
useful and in some absolutely necessary. But, I do not believe it should
be used indiscriminately. Even if side effects are rare, when they arise
they can be serious. Even if the main objective is that recurrence be avoided,
patients, as they often refer, may have an unpleasant subjective perception
of the prosthesis after recovery. I would also like to remark, that even
if a foreign body is biocompatible, it remains artificial and unnatural.
That is why I propose a technique, which is not a return
to the past, but belongs to the "post mesh" era. I think the time
has come to give its due weight to physiology, so often emphasized
yet so often neglected. I also believe that the biology of tissue should
be respected more. Biology is not respected by substituting tissues
with inert foreign bodies, even if sutures are without tension.
Today, the repair of the defense mechanisms and respect
of the biology of tissues can be harmonized.
8
PHYSIOLOGICAL HERNIOPLASTY
INDEX
To understand the principles and objectives of my inguinal
hernia surgical repair technique it is sufficient to refer back to chapter
6.
My technique was devised in 1988 for two purposes:
- restoration of the defense mechanisms of the inguinal
region through repair which adapts the anatomy to functional necessity,
- respect of the biology of sutured tissue.
These two objectives, always considered of major importance,
have never been simultaneously achieved by traditional or modern methods.
The technique
Common preliminary steps

-
The best skin incision is transversal, because it heals better.
-
The cribriform fascia is cut slightly below the inguinal
ligament to free the external oblique aponeurosis on the lateral side and
to check for the presence of a subclinical crural hernia.
-
The external oblique aponeurosis is cut along the fibers
as far as the opening of the superficial ring
-
The medial flap of the external oblique aponeurosis is dissociated
from the layer below. The separation should be quite wide in order to uncover
the rectus sheath as much as possible.
-
The funiculus is isolated at the level of the pubic spine
and pulled laterally.
-
The inferior border of the internal oblique muscle is separated
from the medial fibers of the cremaster (Fig. 8.1).
-
The cleavage between the internal oblique muscle and the
aponeurotic arch of the transversus muscle is detected. The internal oblique
muscle is retracted medially and the layer constituted by the aponeurosis
of the transversus and transversalis fascia, is exposed medially to the
deep ring, for a wide tract.
Treatment of the deep layers
The treatment of the deep layers is different in indirect
hernia with a medium-small defect and in direct or indirect hernia with
a large defect.
Indirect hernia with a medium-small defect.
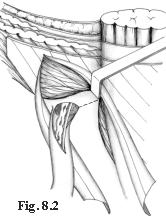
-An incision on the funiculus involving the proximal tract
of the internal spermatic fascia as far as the deep ring, is performed.
-The sac, beyond the neck, is isolated. It can be either
resected or simply pushed into the preperitoneum. I prefer the second choice,
unless the sac is very long and adherent. In this case, I divide it and
leave the fundus in situ.
-The elements of the funiculus (vessels and deferent)
are separated from the proximal tract of the internal spermatic fascia
and cremaster and then isolated. The isolation is extended to the level
of the deep ring and, for a few centimeters, into the preperitoneal area.
-A two-centimeter incision is performed on the transversalis
fascia and aponeurosis of the transversus, starting on the deep ring, in
a medial and cranial direction (Fig. 8.2).
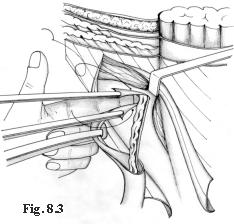
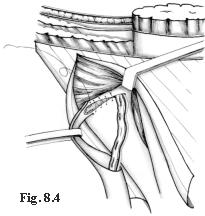
-The elements of the funiculus are brought to
the medial angle of this incision (Fig. 8.3); then, the first layer of
suture is started. With the first passage of the thread, a new easily calibrated
deep ring is created (Fig. 8.4). The incision is then sutured until the
original ring is completely closed (Fig. 8.5). Keeping the same suture,
a second layer is created, but in the opposite direction, to cover the
first layer with the cremaster and internal spermatic fascia. (Figs. 8.5,
8.6).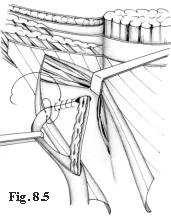

Direct hernia or indirect hernia with a large defect.
My technique consists in partially repairing the posterior
wall of the inguinal canal so as to transform the large defect into a small-defect
indirect one. The surgery is then completed following the repair technique
for a small-defect external oblique hernia.
The common preliminary procedure has already been described.
Having isolated the funiculus and retracted the internal
oblique muscle the rest of the operation will follow a precise pattern
depending on the nature of the hernia.
In indirect hernia, a medial incision is performed,
which involves the proximal tract of the internal spermatic fascia and
the deep ring. A second incision on the transversalis fascia of the deep
ring up to the pubic spine is performed.
In direct hernia, the transversalis fascia above
the hernial sac is resected. Then an incision on the fascia transversalis
is extended cranially up to the deep ring.
The sac, both in direct and indirect hernias, is isolated
beyond the neck and simply pushed into the preperitoneal cavity. Only in
big scrotal hernias is the sac transected leaving the body and fundus in
situ.


-The preperitoneum is detached from the transversalis
fascia medially to the hernial defect, beyond the lateral margin of the
rectus sheath.
-The posterior wall of the inguinal canal is partially
closed through overlapping of the flaps with a continuous suture. The suture
joins the iliopubic tract to the internal surface of the transversalis
fascia at the level of the lateral margin of the rectus muscle (Fig. 8.7).
It starts at the pubic spine and stops at the level of the inferior epigastric
vessels. The left-over medial flap of the transversalis fascia is joined,
using the same continuous suture, to the iliopubic tract. (Fig. 8.8). The
suture does not involve the inguinal ligament and touches only slightly
the deep ring, which is left open.
-Then one proceeds as if dealing with an indirect hernia
with a medium-small defect: the internal oblique muscle is retracted and
an approximately 2-centimeter incision with a medial direction is performed
on the transversalis fascia beginning from the deep ring (Fig. 8.8).
-The elements of the funiculus are separated from the
internal spermatic fascia + cremaster and dislocated to the medial angle
of this incision. A continuous suture creates a deep neo-ring, unites the
borders of the incision and, after the deep primitive ring has been completely
closed, on the way back, covers the suture line with the cremaster. (These
surgical maneuvers have been described in detail; cf Figs. 8.3, 8.4, 8.5,
8.6).
-In cases in which the posterior wall of the inguinal
canal is wide and strong, instead of repairing with an overlaying flap,
a plication of the transversalis is carried out to narrow the inguinal
canal: a continuous suture joins the iliopubic tract to the aponeurotic
arch of the transversus, from the deep ring to the pubis.
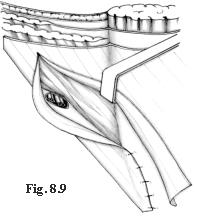
Treatment of the superficial layer
The repair of the superficial layer is the same as in
all hernias.
Cap11
-
The external side of the inferior-lateral border of the external
oblique aponeurosis is freed completely from every adhesion.
-
The point at which the inferior part of the internal oblique
muscle reaches the rectus sheath is found. At this level a new superficial
ring is created: the suture is performed between the margin of the inferior-lateral
flap of the external oblique aponeurosis and the rectus sheath, along a
line parallel and 1 cm medially from the lateral margin of the rectus muscle.
The suture runs up to the pubis (Fig. 8.9), while the funiculus is kept
laterally to the operation field. Therefore, the suture is behind the funiculus.
Usually, we use continuous suture in both directions, so that it is easier
to tie the thread.
-
The funiculus is relocated in its place, leaning completely
on the internal oblique muscle.
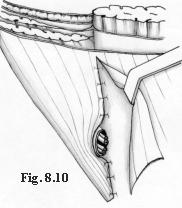
-
Enough space is left for the exit of the funiculus (Fig.8.10),
and a second suture between the rectus muscle sheath and the lateral margin
of the external oblique aponeurosis, along the previous line, is performed.
The third suture level is, therefore, completed.
-
The fourth layer is characterized by the suture which involves
the superior-medial flap of the external oblique aponeurosis and the external
side of the inferior-lateral aponeurotic flap, so that there is wide overlapping
without much tension. This suture level, as the previous one, is antefunicular
and proceeds from the neo- superficial ring to the cranial extreme of the
incision (Fig. 8.11) and retrofunicular from the superficial neo-orifice
to the pubis (Fig. 8.12). In case of the poor-quality tissue, this technique
may include the use of mesh
The suture materials
We use absorbable sutures (polyglicolic acid) and nonabsorbable
sutures (polypropylene). The latter only in cases in which polypropylene
meshes are used.
The main technical details
Isolation of the funicular elements from the proximal
tract of the cremaster
After having opened the internal spermatic fascia, the
isolation of the vessels is very easy. The deferent duct is more adherent
to the surrounding tissues, but easily recognizable because of its consistency.
Usually it is possible to see the peritoneal reflection stuck to the elements
of the funiculus. We dissociate it for a few centimeters to avoid its passing
into the deep ring which might lead to a further hernia. It is necessary
to resect any adipoceles, even the smallest ones, frequently located on
the internal side of the cremaster.
Isolation of the layer: transversalis fascia + aponeurosis
of the transversus muscle
After isolating the hernial sac, two Kelly forceps are
put on the medial border of the deep inguinal ring, next to the preperitoneal
fat, and also a light upward traction is performed. With a Russian forceps,
the adipose tissue below is pinched and pushed inwards. In this way, the
separation of the layers occurs easily. The transversalis fascia can be
well detected at deep level. The Kelly forceps are placed on it with a
light traction. With the Russian forceps itself, held closed and used as
a spatula, the fibers of the internal oblique muscle are easily separated
from the level below. Then they are pulled back medially in order to uncover
the transversus arch widely.
Incision of the transversalis fascia and creation of
new deep ring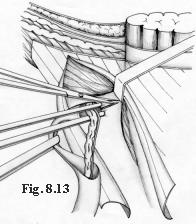
As said, two Kelly forceps are placed on the border of
the transversalis fascia at the level of the deep ring. The caudal forceps
is removed, passed below the funicular elements and reattached at the same
spot. The fascia is kept in traction with the forceps and cut with the
scissors ( Fig. 8.13). At this point, the traction applied to the internal
oblique muscle should be high to better reveal the operation field. A two-centimeter
medial cut is performed. If the internal oblique muscle is poor, the incision
is directed more cranially, so that the new ring can be covered by the
muscle when the retractor is removed. The funicular elements are dislocated
at the inner angle of the cut and pulled medially.
The two Kelly forceps are put close and pulled with the
left hand, palm upwards.
The borders of the incision have to be very close. The
index finger of the same hand, introduced into the preperitoneal space,
pushes the funicular elements on the medial border of the incision. In
this position, the first stitch of the continuous suture is performed (Fig.
8.3), then tied to give the correct calibration to the ring.
Closure of the deep ring
The continuous suture is brought from the neo-ring to
the deep ring. Once the deep ring has been reached, the suture runs along
the external hemicircumference. The inguinal ligament, which is close to
the lateral edge of the deep ring, should not be included in the suture.
The ring will be easily closed by the traction of the thread. The same
suture, on the way back, joins the free part of the cremaster to the suture
line below.
Verification of the ring caliber
The correct caliber of the deep neo-ring and of the superficial
neo-ring are verified introducing a curved Kelly forceps into them. The
deep ring has to be neither too narrow nor loose. The new superficial ring
has to be rather wide. If it is too narrow, it should be widened with a
short transversal incision on the external oblique aponeurosis.
9
THE USE OF MESHES
INDEX
Meshes are a great progress in hernia surgery and may
be useful in some cases, in others indispensable. I do not think, however,
that meshes should be used merely on principle.
In small hernia defects, when the tissue is weak, they
should be used to reinforce sutures and tissues and perform a "barrier-
function", while the defect must always be sutured. Only in large defects
the mesh substitutes tissue. The priority is reduction of passive areas
rather than concern about suture traction. Under strain and in a standing
position tension on the suture is inevitably provoked. Furthermore, endoabdominal
pressure creates stress in the passive areas in proportion to their size.
In primary hernias if the tissues are very weak, inelastic
and lacking in quantity we use meshes to reinforce the hernioplasty. This
occurs in 5% of primary hernia cases. The mesh is positioned in the preperitoneum
or alternately in front of the posterior wall of the inguinal canal and
of the deep ring, once it has been closed. Mesh may also be used for prudential
reasons when the surgeon is not very familiar with the physiological hernioplasty
technique.
We use mesh on principle in crural hernias and in recurrence.
In this case, we try to close (successfully in most cases) or, in any case,
to narrow the hernial defect as far as possible.
In crural and recurrent hernias meshes are always used
and positioned in the preperitoneum.
The use of preperitoneal meshes in primary hernias
 The
procedure is identical to that already described for direct or indirect
hernias up to the step where the sac is isolated. The funicular elements
are separated and well isolated from the cremaster + internal spermatic
fascia.
The
procedure is identical to that already described for direct or indirect
hernias up to the step where the sac is isolated. The funicular elements
are separated and well isolated from the cremaster + internal spermatic
fascia.
A rectangular polypropylene mesh, of about 4 x 8 cm is
used.
A cut of about 2 cm is made at 1-2 centimeters from the
midpoint, perpendicular to one of the longer sides of the mesh. (Fig. 9.1).
The mesh is oriented with the cut side towards the surgeon and the shorter
tract in a cranial position. The cord elements are inserted into the cut,
which is then transformed into an eyelet with 1-2 polypropylene stitches.
(Fig. 9.2).
In the indirect hernia, the mesh is placed in the preperitoneal
area through the incision of the transversalis fascia made to create the
neo-deep ring. The mesh is then fixed to the wall, including it in the
suture of the transversalis fascia.
In large hernias or in direct hernias, the mesh is passed
into the preperitoneal area through the wide incision performed on the
posterior wall of the inguinal canal. During the repair phase, we usually
fix the mesh to the wall, including it in the suture. (Fig. 9.3).
In both cases, the operation is performed following the
same technique, as if the mesh were not used.
The use of meshes in the prefascial area in primary hernias
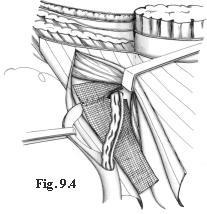 In
indirect hernias, when the transversalis fascia is weak or inelastic and
the closure of the deep ring appears unreliable, a polypropylene mesh of
about 2 x 6 cm is used on the posterior wall of the inguinal canal.
In
indirect hernias, when the transversalis fascia is weak or inelastic and
the closure of the deep ring appears unreliable, a polypropylene mesh of
about 2 x 6 cm is used on the posterior wall of the inguinal canal.
The mesh is positioned after the deep ring is closed.
A short cut is made on the medial side of the mesh at the height of the
neo-deep ring. This cut allows the passing of the funiculus but does not
create a ring around it (Fig. 9.4).
The thread used for suture, with which the deep ring
has been closed, is posterior to and outside the mesh. With the same thread,
backwards, the proximal flap of the cremaster is placed on the mesh, including
the transversalis fascia in the suture.
The mesh is then spread along the posterior wall of the
inguinal canal. The parts of the mesh that exceed the medial and cranial
sides, are to be positioned under and not anterior to the internal oblique
muscle.
Other anchoring stitches are not necessary. Then, the
repair of the overlapping flaps of the external oblique aponeurosis is
performed.
The use of meshes in large inguinal and crural hernias
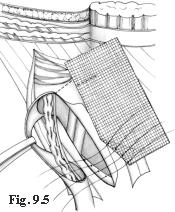 Our
approach is usually inguinal. We reach the preperitoneum and the Cooper
ligament, once the posterior wall of the inguinal canal has been opened.
Our
approach is usually inguinal. We reach the preperitoneum and the Cooper
ligament, once the posterior wall of the inguinal canal has been opened.
The polypropylene mesh has a rectangular shape of about
6-8 cm x 10-12 cm. The inferior-lateral angle of the mesh is folded so
that the length and inclination of the edge of the lapover fits the Cooper
ligament and so that the long side of the mesh is parallel to the axis
of the groin.
A set of separate stitches is passed through the Cooper
ligament and the mesh, at the level of the folded area.
Three- four stitches of monofilament polypropylene begin
from the pubis and proceed laterally along the Cooper ligament, almost
as far as the femoral vein. (Fig. 9.5). The suture on the Cooper ligament
is performed more easily if the surgeon moves on the other side of the
operation field.
The mesh is passed loosely in front of the femoral vessels
so that the femoral vein does not undergo compression even when it is swollen
as in the standing position. A suture unites the mesh to the iliopubic
tract and to the deep border of the inguinal ligament.
Before the suture has been completed, the funicular elements
are passed through an eyelet created on the mesh.
The mesh is laid in the preperitoneal area.
The further steps depend on the conditions encountered.
In most primary hernias, hernioplasty can be performed as described for
direct hernia, anchoring the mesh to the suture of the deep layer.
In recurrence, if necessary, the mesh is sutured to the
transversalis fascia corresponding to the posterior wall of the rectus
muscle. The stitches are positioned parallel to the mesh and 1-2 cm away
from medial border. As far as possible the wall is repaired; in any case
the aim is to narrow the opening as much as possible and cover the mesh
with the upper layers.
The use of meshes in crural hernias
Large crural hernias are repaired anchoring the mesh to
the Cooper ligament with the above-mentioned technique.
The anterior approach in the crural hernia is simple,
but we cannot obtain a good repair directly suturing the hernial defect.
The Cooper ligament and the transversalis fascia are very difficult to
reach through a small hernial defect. Then the lack of tissues and their
stiffness do not allow the performance of a good suture. Therefore the
use of mesh is necessary.
I have developed a technique called "Locked -Plug".
It is very easy to perform and it permits us to treat crural hernias having
a small diameter (1-2 cm) availing of an anterior approach. This technique
can be used also to treat subclinical crural hernias found during an operation
for inguinal hernia. In this case, the crural hernia is repaired independently
of repair for inguinal hernia.
The "Locked-Plug" technique

The approach is anterior. Once the cribriform fascia has
been opened, the hernial sac is reached, reduced or resected.
It is important to detach the sac itself from the hernial
defect. A polypropylene square of 4 x 4 cm is cut. A thread of monofilament
polypropylene is passed through the central point of the square and tied.
The end of the thread (the part beyond the knot) is left 10 cm long and
is not cut.
The square-shaped mesh is folded twice along the orthogonal
lines, crossing the center (Fig. 9.6), so that the thread remains on the
inside.
Then the mesh is bent diagonally to give it a cone shape
in which the tip corresponds to the midpoint. The "cone" is then fixed
with a curved Kelly forceps and introduced into the hernial defect (Fig.
9.7).
When the forceps is removed, the cone tends to expand
spontaneously helped by the forceps re-introduced into the defect, while
a slight traction is applied on the thread.
The same thread is used to suture the borders of the
hernial defect. Two stitches are sufficient (Fig. 9.8).
A traction on the tract of the thread linked to the needle
narrows the defect and fixes the mesh onto it.
The two ends of the thread are then tied together.
It is not necessary to include the Cooper ligament and
the iliopubic tract in the suture, which cannot be reached through the
small defect. It is sufficient to suture the inguinal ligament to the pectineal
fascia.
The purpose of the operation is to narrow the outlet
of the canal and plug it with a well-anchored mesh. The holes made by the
stitches, even if they were to widen, are protected by the mesh itself.
Tension of the suture is minimal
The procedure is easy and secure: the suture is limited
to the central area of the hernial defect only, at a secure distance from
the femoral vein.
The use of meshes in inguinal recurrences
The treatment of recurrence requires great specific surgical
experience, not only in the repair, but also in the dissection phases and
in the preparation of the layers and of the spermatic cord.
In the past years, we have chosen to minimize dissection
and results have proven us to be right. We have limited dissection only
to the preparation of the sac and the hernial defect, and in indirect hernias,
to the funiculus. If hernias are multiple and well separated, we treat
each separately.
This repair always requires the use of mesh.
We use different repair techniques depending on whether
we are dealing with:
-
direct hernia with a small defect
-
direct hernia with a medium defect
-
indirect hernia
-
hernia with a large defect
Direct recurrent hernia with a small defect (up to 1 cm
in diameter)
As in crural hernias, this repair is performed with the
Locked-Plug technique.
Direct recurrent hernia with a medium defect (1-3 cm
in diameter)
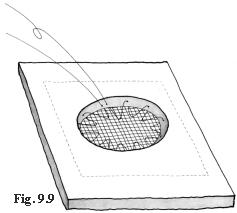 Once
the sac has been pushed into the peritoneal cavity and the defect is freed
from tissue adhesions, a mesh bigger than the hernia defect is positioned
in the preperitoneum. A continuous suture joins the mesh to the lower part
of the wall without passing through its entire depth. The suture then runs
along the border of the hernial defect and describes a circle of smaller
diameter on the mesh. (Fig. 9.9).
Once
the sac has been pushed into the peritoneal cavity and the defect is freed
from tissue adhesions, a mesh bigger than the hernia defect is positioned
in the preperitoneum. A continuous suture joins the mesh to the lower part
of the wall without passing through its entire depth. The suture then runs
along the border of the hernial defect and describes a circle of smaller
diameter on the mesh. (Fig. 9.9).
Once the suture has been completed, the thread is pulled
and tied up. This round suture fixes the mesh and narrows the hernial defect,
while at the same time it avoids that the preperitoneal fat enter between
the mesh and the wall.
Then another suture joins the edges of the hernial defect.
This suture is carried out only when there is no excessive traction and
includes only the superficial level of the wall.
Indirect recurrent hernia with a small - medium defect
(1-3 cm in diameter)
In indirect hernias, once the hernial defect and the
funiculus have been prepared, one mesh bigger than the hernial defect is
prepared.
The spermatic cord is passed through the mesh through
a 2-cm cut and a suture is performed, so that a calibrated ring is created.
The mesh is introduced into the preperitoneum through
the hernial defect.
If the defect is small, it can be sutured directly, calibrated
on the spermatic cord and the mesh included in the suture.
If the defect is medium sized, a circular suture between
mesh and wall is performed, as described for direct hernia. In this case,
if there is not much tension, the hernial defect is sutured and calibrated
on the funiculus.
Hernia recurrence with a large defect (more than 3
cm in diameter)
Fortunately, hernia recurrences with large defects, associated
with lack and stiffness of the tissues, are very rare. In this case, it
is impossible to standardize a procedure: it requires surgical experience
and ability. If the surgeon is not familiar with the preperitoneal approach,
it is better to anchor the prosthesis to the Cooper ligament as described
above. The mesh must be considerably larger than the hernial defect. Therefore,
a wide dissection of the peritoneum and the ligation of the inferior epigastric
vessels are necessary.
10
CASES AND RESULTS
INDEX
Francesco Guarnieri
From December 1988 to June 1999, we operated on 2,326
patients for inguinal and crural hernia: 1,246 for indirect hernia, 470
for direct hernia, 335 for double hernia, 226 for recurrent hernia, 49
for femoral hernia. During these operations 47 subclinical femoral hernias
(2%) were found.
2,162 were males, 164 were females; the average age was
56 years (min. 1, max 98).
Local anesthesia was used on 1,710 patients (74 %), general
anesthesia on 421 patients, spinal anesthesia on 195 patients (8%). The
choice of the type of anesthesia to be used was decided with the patient.
Primary direct and indirect hernias
From the onset physiologic hernioplastic technique was
applied in 2,051 operations. This technique has undergone a series of marginal
technical variations over time. The most significant change has been the
percentage variation in the use of mesh as a reinforcement in hernioplasty.
Up to January 1998, when meshes were used, these were positioned in the
preperitoneal space only. Subsequently prefascial meshes were also employed.
During the first year meshes were used in 49% of all
cases. This high percentage was linked to the fact that we were not as
yet certain of the efficacy of the new technique. As the results grew increasingly
encouraging, we started to reduce the use of meshes drastically. In the
second year we used meshes in 50% of those cases we considered as being
high risk due to poor tissue quality. Since no significant incidence of
recurrence occurred, the use of meshes was gradually reduced to 8% in 1991.
The decision whether to use meshes is usually made in the operating theatre,
where the quality of the tissues can be evaluated.
Another important variation is the execution of incisions
to relax the rectus sheath, which technique we eliminated in February 1996,
having verified through ultrasound and CAT that no significant widening
of the rectus muscle occurred.
Today we use the relaxing incision of the rectus sheath
in those extremely rare cases when the rectus muscle is very narrow.
Recurrent hernias
Recurrent hernias belong to a heterogeneous group of cases
where physiological hernioplasty is difficult to perform due to fibrosis.
Moreover, in the last few years we have reduced dissection to a minimum.
As already stated, in recurrent hernias we always apply
meshes.
The Locked-Plug
The Locked-Plug was not only used in crural hernias, but
in other kinds of hernias where the defect always presents a diameter of
less than 2cm. We have used it in 218 cases: 96 femoral, 57 recurrent,
30 umbilical and epigastric, 23 incisional, and 12 Spigelian hernias. We
have treated 47 subclinical crural hernias, detected during surgery for
inguinal hernia, with the Locked-Plug.
Follow-up
Since December 1988, patients have been scheduled for
follow-up after 7 days, 1 month, 1 year and then annually. Patients who
have not followed follow-up programs have been excluded from this survey.
Primary hernias
Here we shall speak mainly about primary hernias. The
technique has been applied systematically only in this ambit. Postoperative
complications that arose were: 5% subcutaneous seroma, 1 % temporary testicular
edema, 0.7 % hematomas, 0.4% wound infection, 0.1% testicular atrophy,
0.6 % recurrence. It should be noted that no recurrence occurred in those
cases where meshes were employed.
In the first year, when the femoral ring was not systematically
explored, 2 cases of crural pseudo-recurrence were found. After that no
cases of pseudo-recurrence were observed. Subclinical crural hernia was
found in 2% of patients operated for primary hernia.
Recurrent hernias
Complication incidence rates: 0.8 % suppuration, 14 %
subcutaneous seroma, 2 % hematomas, 2% testicular edema, 1.5% testicular
atrophy, 2.6% new recurrence.
LockedPlug
Complications: 6% subcutaneous seroma.
No recurrence.
11
RATIONALE
INDEX
My rationale is best understood in the light of Chapter
6. As stated there, this technique aims at restoring the architecture of
the inguinal region, so that the defense mechanisms are repaired and the
weak areas narrowed and reinforced.
The objective is not to restore the anatomy, but adapt
it to functional needs, compensating for tissue weakness while fully respecting
the norms of physics and biology.
The characteristics of the technique are:
- elimination of the deep inguinal ring and creation
of a neo-orifice.
- narrowing and shortening of the inguinal canal, adapted
to fit the internal oblique muscle.
- overlap of the external oblique aponeurotic flaps.
- preservation of the cremaster
The elimination of the deep and construction of the new ring
In most cases the deep ring is surrounded by weak tissues
unable to resist suture strain. Its reconstruction usually proves quite
untrustworthy. For this reason almost all herniorrhaphy techniques seek
to reinforce the deep ring and anchor it to the inguinal ligament, thus,
immobilizing, stiffening and defunctionalizing it.
Besides, the deep ring is not clearly detectable unless
the cremaster is cut. Tissue weakness, together with defunctionalization
and an inexact suture, are among the chief causes of recurrence.
For this reason we have chosen to create a neo-deep ring
which may be easily calibrated around the funicular elements and positioned
in a stronger zone where it can be protected by the internal oblique muscle.
When the transversus muscle contracts, the neo-ring narrows and rises,
because it is situated between the fibers of the aponeurotic arch. The
sphincter effect is thus repaired.
The narrowing and shortening of the inguinal canal
As stated above, the shutter mechanism is obtained only
when the inguinal canal is narrow and totally surrounded by the internal
oblique muscle.
In hernia patients the internal oblique muscle is almost
always hypotrophic and reaches the rectus sheath "high" relative to the
pubic spine. The lower zone, unprotected by the muscle, is called the inguinal
triangle (Fig. 6. 3). The suture
of the external oblique aponeurosis onto the rectus sheath is performed
so that the inguinal triangle is excluded from the inguinal canal and reinforced
(Fig. 8.9). Consequently, the
inguinal canal becomes shorter, but functional. The shutter mechanism is
thus achieved also because the internal oblique muscle is not affected
by stitching capable of limiting its movement.
Overlapping the external oblique aponeurotic flaps
The external oblique aponeurosis is elastic and pliable
along the fibers transversal axis. By suturing the external aponeurotic
flap to the rectus sheath, a narrowing of the inguinal canal and of the
inguinal triangle characterized by a moderate degree of suture traction,
is produced. The medial flap is brought to overlap the lateral one abundantly,
producing a minimum amount of tension. This overlaying distributes the
already moderate suture traction even more and creates an extensive and
compact scar area, which prevents the external oblique aponeurosis from
fraying. Consequently, this aponeurotic layer, as a veritable biological
prosthesis, creates new compact scar tissue which reinforces the passive
areas without tension of the sutures.
The greatest advantage is obtained at inguinal triangle
level, a passive area where traditional methods frequently encounter recurrence.
In the inguinal triangle the lateral flap of the external oblique aponeurosis,
without the intrusion of the funiculus, is placed directly on top of the
transversalis fascia, with which it forms an adherent cicatricial plane.
The medial flap of the aponeurosis is overlapped once more forming a second
uletic plane. Together, these create a strong wall, certainly no less strong
that one produced by a mesh.
Preservation of the cremaster
According to this technique the proximal portion of the
cremaster + the internal spermatic fascia, free from the funicular elements,
is overlapped onto the suture on the transversalis fascia between the deep
ring and neo-ring. The cremaster, besides reinforcing the suture, completely
and securely occludes the deep ring and blocks any small lacerations which
may arise at the passage of the stitches on the transversalis fascia below.
Further below, the cremaster remains intact and protects the testicular
vessels from risks of iatrogenic lesions in case of an operation for recurrence.
In addition, resection of the cremaster may lead to neuralgia
of the genital nerve. The cremaster vessels also guarantee a collateral
vascular bed in cases of testicular vessel lesions.
Discussion
On the basis of what we have stated several times above,
this technique is highly efficient in repair of the functionality of the
inguinal canal. Even if the sling mechanism of the deep ring is not restored,
the results prove that the sealing function of the posterior wall, at neo-ring
level, remains intact. In fact the hernia recurrences we have encountered
after our technique have never occurred at neo- deep ring level.
As to the narrowing of the posterior inguinal canal wall,
until February 1996 we supported the idea of the rectus sheath relaxing
incision and performed it systematically. We held that this relaxing incision
served to expand the rectus muscle laterally and narrow the inguinal canal.
We were not interested in reducing the suture tension between the external
oblique aponeurosis and the rectus sheath, which we considered minimal.
After systematic examinations availing of ultrasound and CAT scans we discovered
that lateral expansion of the rectus muscle did not in fact occur. We therefore
eliminated the relaxing incision, which choice produced no changes in either
postoperative conditions or results. At the same time we paid greater attention
to the question of freeing the lateral flap of the external oblique aponeurosis
from the lateral fascial tissues to bring it closer to the rectus muscle.
The technique does not favor the formation of crural
hernias. We registered 2 crural pseudo-recurrences among patients operated,
in the first period, when the fossa ovalis was not as yet explored. Since
we began systematically exploring the fossa and treating subclinical concomitant
crural hernias (2% of the cases), no pseudo recurrence has arisen.
The problem of suture tension and the poor healing, (which
worries the supporters of the "tension free" school) need to be addressed.
In our method the suture lines invest only a tiny quantity
of tissue and are used solely to connect fascias (which do not devascularize);
furthermore, they are not aligned, nor do they pass through the entire
thickness of the wall, thus receiving protection from the upper and lower
layers which act as a barrier. The suture lines on the external oblique
aponeurosis are arranged in such a way as to distribute the already low
tension. The overlap of the flaps creates ample contact areas between surfaces
developing a solid scar tissue, similar to those around meshes, between
them. Outcome data accruing to primary hernia operations reveal that this
technique has a low recurrence rate, the lowest for techniques not availing
of prosthetic mesh. The recurrences encountered by us were all direct smalldefect
hernias at either original deep ring level or immediately below it.
Postoperative complications such as suppuration, transitory
testicular edema and testicular atrophy comply with most reports.
It is very difficult for any author, however self-critical,
to point out the disadvantages of his/her own method. As similar self-criticism
is hardly credible, I shall here present a number of critical objections
I have received in a series of questions and answers.
In your largehernia technique does the hernia
defect repair not resemble Shouldices?
This method and Shouldices are very different both theoretically
and practically; they are similar only in the repair of the lower part
of the inguinal floor in direct hernias.
Does excessive traction between the rectus muscle and
the iliopubic tract not occur?
The rectus muscle and the transversalis fascia are very
flexible. Besides, the already moderate amount of suture tension existing
is reduced by the sutures above. Furthermore, it involves the tract between
the lower epigastric vessels and the pubis where there is less distance
between the edge of the muscle and the iliopubic tract.
The funiculus forms a Z-shaped path. Does this not
affect the blood supply to the testicle?
The sinuosity of the path of the vessels does not impede
the blood flow. In fact, the incidence of transitory edema (2%) and testicular
atrophy (0.1%) in males operated on for primary hernia is low and in keeping
with authoritative reports.
Is the funiculus not too tight in the new inguinal
canal, occupied as it is now by the internal oblique muscle?
When the muscle tissue is at rest, it is soft and compresses
the small vessels only slightly, as per Laplace's law. The contraction
of the muscle undoubtedly causes compression, but it is temporary and irrelevant.
Besides, under normal conditions, the contraction of the internal oblique
muscle presses the funiculus.
Is the shortening and reduction of the obliqueness
of the inguinal canal not in contradiction with physiology?
Obliqueness and the shortening of the inguinal canal
do not seem to me to be of any great physiological relevance. I believe
that it is important that the deep and superficial rings not be aligned,
but staggered by 2-3 cm, so that the external oblique aponeurosis may effect
the lower anatomic layers synergistically. What really counts is repairing
the defense mechanisms.In my technique the rings are never aligned, even
when the internal oblique muscle is inserted high on the rectus sheath,
because in this case the neo-deep ring is created in a position decidedly
more cranial and medial compared to the original one.
McVay and Anson underlined the importance of repairing
the anatomical planes and avoiding repair between different levels. Do
you agree?
My intention was to repair physiology not anatomy. Nevertheless,
I can say that my repair is actually much more anatomical than it may appear
to be.
Are the sutures between the two flaps of the external
oblique aponeurosis not under traction?
The external oblique aponeurosis is transversally very
elastic. The sutures are executed in such a way as to avoid excessive traction
and stress due to muscular contraction. The external oblique muscle contracts
longitudinally and not transversally with respect to the suture line. Scarring
is not impeded by the moderate tension of the suture, also because the
aponeurosis receives a scarce blood flow and is, therefore, not subject
to ischemia.
Is there not traction on the inguinal ligament with
consequent risk of iatrogenic crural hernia?
The risk of iatrogenic crural hernia is minimal even
in techniques like Shouldices, which perform direct sutures along the
whole inguinal ligament. Much has been written about this point.In my technique
only the most superficial part of the inguinal ligament is barely involved
and in no way subjected to transversal traction. I can also say that since
I began exploring the crural ring, I have never encountered crural pseudo-recurrences
in my patients, while I have come across subclinical crural hernias in
about 2% during primary hernia operations.
The technique seems to be complicated and rather difficult
to learn and perform. Do you not agree?
I also have the impression that this technique is not
easily grasped and cannot really explain why. For some reason, some surgeons
appear to learn it immediately, while others do not. It may depend on a
surgeons ability to free him/herself from traditional schemas. However,
once the technique has been understood it is not difficult to perform.As
far as " the feasibility" of the technique is concerned, two elements are
important:
-
the average operating time in my unit is about 30 minutes
which indicates that the performance of the technique is not so complex
-
neither recurrence nor significant complications occurred
among the first patients operated availing of this technique. They represent
a consistent group of patients who underwent the techniques entire experimentation
and improvement cycle. This fact corroborates the opinion that the clarity
of each phase of the procedure reduces the risk of error to a minimum.
Is it not too much to use such a complicated technique
in the case of simple hernias: should it not be for complicated cases only?
Even the simplest hernias may recur. Hernias should never
recur! I can understand a congenital hernia in a baby or in youths with
a strong wall, cases which, in fact, I treat differently. But in most primary
hernias, this physiological and versatile technique is quite appropriate.
In indirect hernias, the possibility of small associated
direct hernias always exists. Might a technique which does not attempt
systematic repair of the posterior wall of the canal not miss them?
A systematic exploration of the fossa ovalis is always
carried out to ensure that subclinical crural hernias do not exist. The
same is true of the posterior wall of the canal where even tiny hernias
of the fascia transversalis are easily detected.I have often located very
small hernias on the rectus muscle near the pubis. They are located medially
and might be missed even when the posterior wall of the canal is repaired.
In my technique they are occluded by the external oblique aponeurosis.
However they are easily recognizable. All one has to do is look.
Does this technique not produce more postoperative
pain that techniques employing tension-free meshes?
I am not in a position to compare mine with tension-free
mesh techniques. What I can say is that compared to other traditional methods,
this technique drastically reduces postoperative pain as is shown by the
limited use of painkillers: required by 35% of the patients only. Even
postoperative recovery is very rapid. After one week the majority of the
patients are able to move without any problem.
INDEX
References
AMID P.K. et al.: Femoral hernia resulting from inguinal
herniorrhaphy: the "Plug" repair. Contemp. Surg. 39: 19-24, 1991.ASMUSSEN
T., JENSEN F. U.: A follow-up study on recurrence after inguinal hernia
repair. Surg. Gynecol. Obstet. 156: 198-200, 1983.
BERLINER S.D.: Adult inguinal hernia. Pathophisiology
and repair. Surg. Annu. 15: 307-329, 1983.
CANNON D.J., READ R.C.: Metastatic emphysema. A mechanism
for acquiring inguinal herniation. Ann. Surg. 194: 270, 1981
CONNER W.T., PEACOCK E.E.: Some studies on the etiology
of inguinal hernia. Am. J. Surg. 126: 732-736, 1973.
FASIANI G.M., CATTERINA A.: Scritti di chirurgia erniaria.
Tipografia del Seminario di Padova, 1937.
GLASSOW F.: Recurrent inguinal and femoral hernia. Brit.
Med. J. 1: 215-219, 1970.
GREENBURG A.G.: Revisiting the recurrent groin hernia.
Am. J. Surg. 154: 35-40, 1987.
GUARNIERI A. et al.: A new technique for indirect inguinal
hernia repair. Am. J. Surg. 164: 70-73, 1992
GUARNIERI A., GUARNIERI F. MOSCATELLI F.: The functional
repair of inguinal hernia. Hernia 1: 117-121, 1997
GUARNIERI A.: La nuova chirurgia dell'ernia. Masson Milano1995
GUARNIERI A.: Procédé original de plastie
"fonctionnelle" des hernies inguinales primaires. Chirurgie 122: 534-538,
1997
LICHTENSTEIN I.L. et al.: Pain after hernia surgery:
how to prevent it,, how to treat it. Contemporary Surgery 33: 18-22, 1988.
LICHTENSTEIN I.L.: Herniorrhaphy. A personal experience
with 6321 cases. Am. J. Surg. 153: 553-559, 1987.
NYHUS L.M. et al.: Inguinal hernia. Current Problems
in Surgery, Vol. XXVIII, No. 6 June 1991.
NYHUS L.M., CONDON R.E. Eds.: Hernia.
Lippincott Co., Philadelphia, 1995.
PEACOCK E.E., MADDEN J.W.: Studies on the biology and
treatment of recurrent inguinal hernia. Morphological
Changes. Ann. Surg. 179: 567-571, 1974.
PIETRI P., GABRIELLI F.: Il problema delle recidive nella
chirurgia dell'ernia inguinale. Arch. Atti Soc. Il. Chir. 87' Congr., Torino,
1985, p. 59-79.
POSTLETHWAIT R.W.: Recurrent inguinal hernia. Ann. Surg.
202: 777-779, 1985.
READ R.C., McLEOD P.C.: Influence of a relaxing incision
on suture tension in Bassini's and McVays repairs. Arch. Surg. 116: 440-445,
1981.
READ R.C.: Attenuation of the rectus Sheath in inguinal
herniation. Am. J. Surg. 120: 610-614, 1970.
READ R.C.: Properitoneal herniorrhaphy,: a historical
review. World J. Surg. 13: 532-539, 1989.
READ R.C. YODER G.: Recent trends in the management of
incisional herniation. Arch. Surg. 124: 485-488, 1989
RIVES J., NICAISE H.: Hernies inguinales. Encyclopédie
Medico-Chirurgicale, vol. 1 App. digestif 40105-40110, 1978.SCHUMPELICK
V. et al.: Repair of recurrent inguinal hernia. Tactics, technic and results.
Chirurg 61: 526-529, 1990.
SHANDALAKIS J.E. et al.: Surgical anatomy of the inguinal
area. World J. Surg. 13: 490-498, 1989.
SHULMANN A.G. el al. The "Plug" repair of 1402 recurrent
inguinal hernias. 20- Years experience. Arch. Surg. 125: 265-267, 1990.
STOPPA R. et al.: Complications des réparations
prothétiques des hernies de l'aine. Chirurgie, 113: 195-204, 1987.
THOMAS S.M., PEYTON BARNES J: Recurrent inguinal hernia
in relation to ideal body weight.
Surg. Gynecol. Obstet. 170: 510-512, 1990.
WAGH P.V., READ R.C.: Defective collagen synthesis
in inguinal herniation. Am. J. Surg. 124: 819-822, 1972.
YOUNG D.V.: Comparison of local spinal and general anesthesia
for inguinal herniorrhaphy. Am. J. Surg. 153: 560-563, 1987.
APPENDIX
12
THE"SANDWICH"
TECHNIQUE IN INCISIONAL HERNIAS
INDEX
This method was published by me in "Atti della Societa'
Italiana di Chirurgia" in 1988, and later, in 1991, it appeared in the
World Journal of Surgery as an original method by Matapurkar. This is a
technique particularly suited for the treatment of multiple incisional
hernias and cases where the hernial defect is rigid due to fibrosis of
the wall. Normally the mesh is a must but it means creating contact between
the mesh, the bowel and subcutaneous tissue, with greater consequent risk
of complication. The "Sandwich" technique permits that the mesh be isolated
from them, because the prosthesis is located between the two flaps created
by the division of the hernial sac into two parts.
Incisions
Excision of the skin and subcutaneous tissue is generally
preferred; this is performed by carrying out two incisions externally to
the neck of the hernia sac, on scarfree tissue. In this way, the scar
area which surrounds the sac is avoided and the fascial layer is easily
reached. Following this level, the hernial defect and the sac which is
neither resected nor opened until it has been isolated completely, are
easily reached.
Treatment of the sac
In incisional hernias, the sac is a continuation of the
aponeurotic muscular plane from which it may not be separated. As stated,
the sac should not be resected; it is isolated as far as the neck and then
divided longitudinally into two halves, perpendicular to the wall (Fig.
12.1). The adhesions are eliminated for a wide tract of the parietal peritoneum
and the contents of the sac is pushed into the abdomen.
The "Sandwich " repair
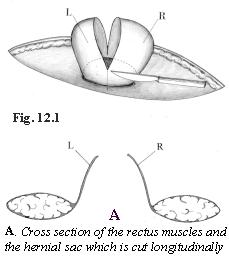
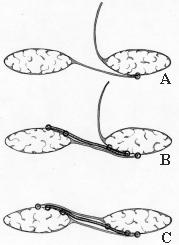
The longitudinal division of the sac creates two flaps
(Fig. 12.1A).The free edge of the flap on the surgeons side of the patient
is positioned inside the hernial defect and is sutured to the parietal
peritoneum along the entire free hemicircumference facing the insertion
(Fig. 12.2A). The suture continues using absorbable synthetic thread, and
is carried out at the greatest possible distance from the neck and includes,
even if only partially, the muscular plane above it.A polypropylene mesh
is shaped to the outline of the hernial defect, exceeding its diameter
by 4 cm.. The hemicircumference on the side opposite the surgeon is fixed
to the parietal peritoneum with a non-absorbable continuous suture concentric
to the previous one.The other hemicircumference is sutured to the premuscular
fascial layer (externally to the hernial defect).A third continuous suture
is carried out with non-absorbable thread to anchor the mesh to the edge
of the hernia defect (Fig. 12.2B).The second flap of the hernial sac (opposite
the surgeon) is pulled over the mesh, so as to cover it completely (Fig.
12.2 C). The free hemicircumference is fixed on the outside of the mesh
at fascial layer, using the absorbable thread employed for the first suture.
INDEX